These sessions, which fulfill the Michigan Department of Licensing and Regulatory Affairs (LARA) “implicit bias training requirement,” have little to do with improving patient care and everything to do with advancing a particular ideological agenda.
The first red flag appears immediately in the module “DEI: Past, Present and Future.”
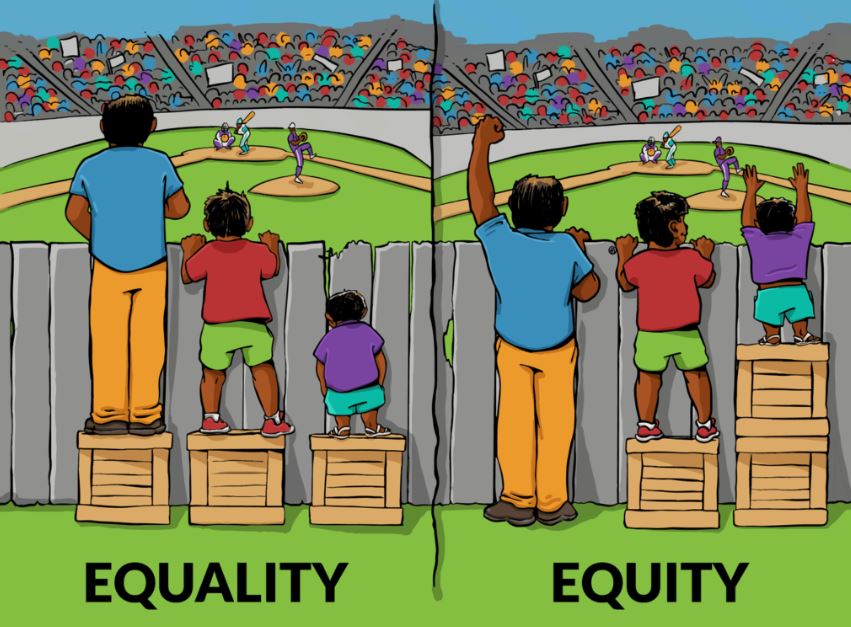
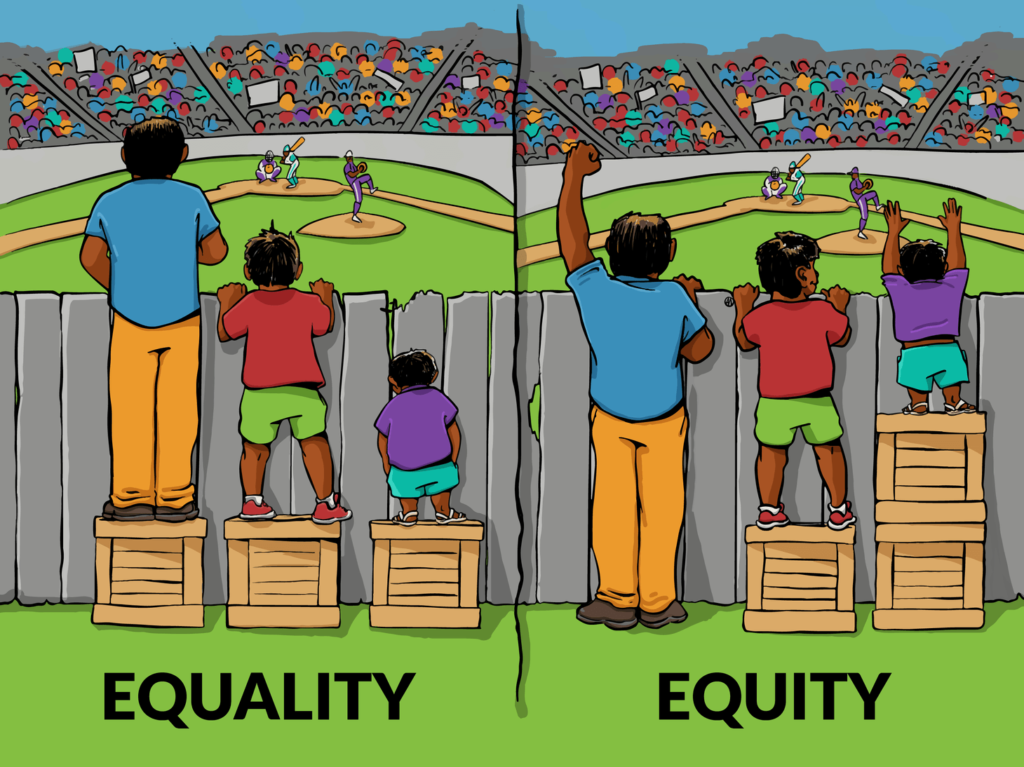
The module begins by comparing DEI to a “party”: diversity is being invited to a party, inclusion is being asked to dance, and equity is “leveling the playing field” and “dancing without barriers.” Accompanying this is the misleading illustration of children on boxes watching a baseball game.
But here’s what’s missing: in practice, “equity” here means discriminating based on race and other immutable characteristics to achieve predetermined outcomes. The Civil Rights Act of 1964 explicitly prohibits such discrimination, a fact the training materials themselves acknowledge when citing the Act and Executive Orders 10925and 11246.
The irony is apparently lost on the presenters.
Later in the presentation, we encounter this little tidbit: race has become “ambiguous” because it’s now about one’s internal self-identification and has lost any degree of objectivity.
Let’s think this through. If race is whatever someone identifies as, then why can’t anyone identify as anything that advantages them? And if they can, doesn’t that render the entire DEI framework meaningless?
One can’t simultaneously claim that racial categories are socially constructed fictions and use them as the basis for medical policy and resource allocation.
The training also includes “The Gardener’s Tale” video, adapted from Dr. Camara Jones, meant to illustrate “institutional racism” via the analogy of a gardener who prefers red flowers over pink, and therefore grows the red flowers in more fertile soil.
It patronizes black Americans by suggesting they cannot succeed without external intervention to overcome systemic barriers – barriers that, conveniently, only the DEI apparatus can identify and remedy.
This paternalistic approach is deeply condescending. It treats minority patients not as autonomous adults capable of navigating the healthcare system, but as victims requiring constant accommodation.
Scholars such as John McWhorter have pointed out that this methodology treats concepts like systemic racism more like a religion than a working theory about society, and in so doing, ignores the multitude of factors – such as personal choice, biological factors, and medical comorbidities – that lead to disparities.
Understanding the true causes of outcome disparities, for example, matters in the context of healthcare and requires moving past the simplistic assumption that all difference is the product of “systemic racism.”
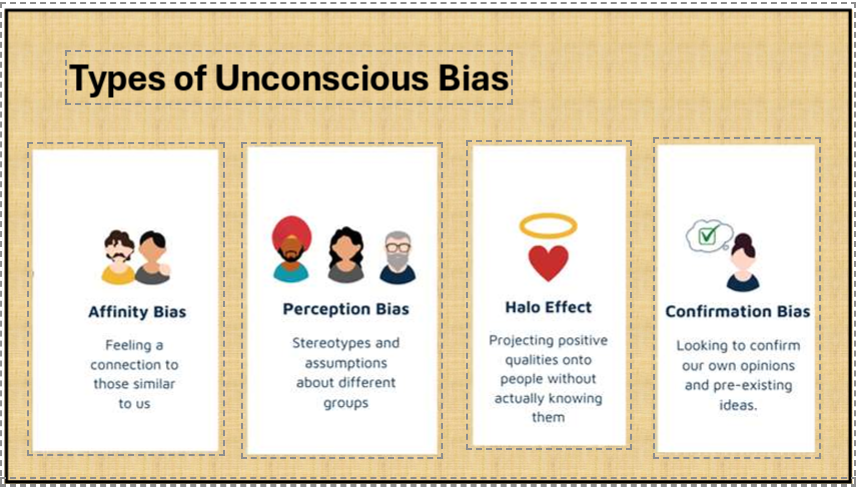
Additionally, the module on “Implicit Bias and its Impact on Health Equity” lists several types of unconscious bias: affinity bias, perception bias, the halo effect, and confirmation bias.
Figure 2. From “Implicit Bias and its Impact on Health Equity.”
When discussing implicit bias, the training cites the Implicit Association Test (IAT) as evidence of bias.
Figure 3. From “Implicit Bias and its Impact on Health Equity.”
However, the IAT has been thoroughlydebunked as a predictor of discriminatory behavior. Even its creators have backed away from strong claims about its validity. Yet here it is, presented uncritically as scientific fact in physician training.
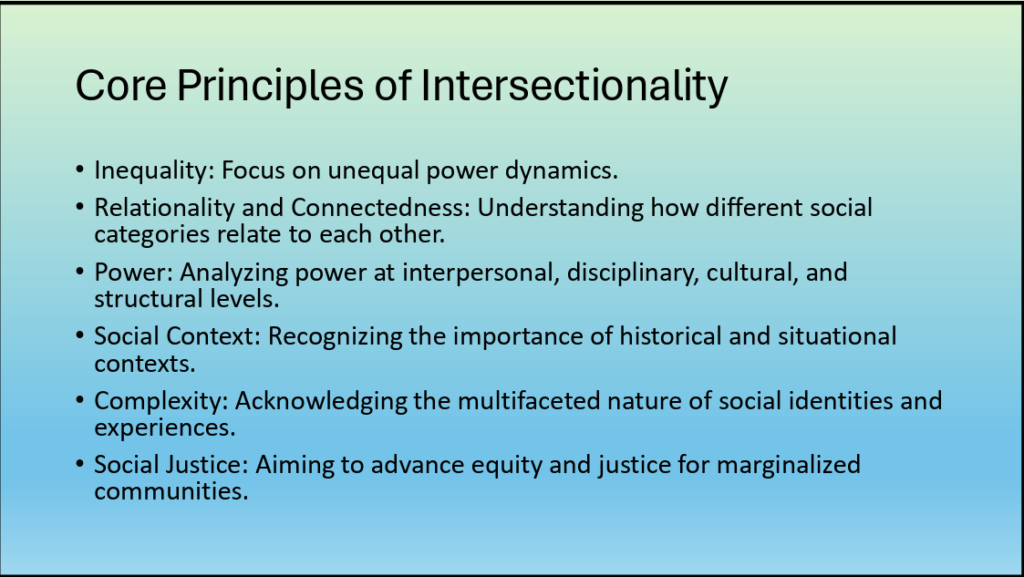
The module “Beyond Equity, Diversity, and Inclusion: The Power of Intersectionality in Addressing Bias” takes things even further. Slide after slide smuggles in radical ideology under the guise of healthcare improvement.
“Intersectionality” – a framework borrowed from critical theory that is used to combine different categories of how one identifies, such as being a certain race, religion, and sexuality – is presented as an established fact.
Figure 4. From “Beyond Equity, Diversity, and Inclusion: The Power of Intersectionality in Addressing Bias.”Figure 5. From “Beyond Equity, Diversity, and Inclusion: The Power of Intersectionality in Addressing Bias.”
These ideas explicitly advance a vision of healthcare that treats individuals in accordance with their group identity, and one in which the pursuit of social justice is central to shaping care within that framework.
So much for doctors focusing on their trade of providing good, quality medical care; now they’re called to be social justice warriors.
What is particularly concerning is that these training sessions represent thousands of hours of physician time and mental energy diverted from actual medical education and patient care. Instead of learning about the latest clinical evidence or honing diagnostic skills, Michigan physicians are subjected to ideological indoctrination that treats them as presumptively bigoted and in need of political re-education.
The presentations, taken as a whole, indicate a clear desire to radicalize participants rather than educate them. For example, it treats any attempt to restrict these divisive DEI programs as a sort of bogeyman; as if it would be disastrous to curb their efforts, but no evidence is given to back up this notion.
Figure 6. From “Beyond Equity, Diversity, and Inclusion: The Power of Intersectionality in Addressing Bias.”
At one point, the materials state: “Health professionals must increase their awareness of anti-DEI misinformation and propaganda, and communicate clearly about the tremendous value of diversity, equity, inclusion, and antiracism.”
Figure 7. From “Beyond Equity, Diversity, and Inclusion: The Power of Intersectionality in Addressing Bias.”
Translation: anything opposed to the standard line about DEI is misinformation and propaganda, and healthcare professionals should not entertain the possibility of another theory.
Is that how medical science is advanced – through dismissing competing ideas as misinformation?
The Michigan State Medical Society should ask itself a simple question: Are Michigan patients receiving better healthcare because their physicians attended these training sessions? That’s doubtful, particularly given the lack of supporting evidence.
What’s clear is this: Medical care should be based on clinical evidence, individual patient needs, and the physician’s judgment – not on contested theories about social construction, intersectionality, and systemic oppression. Our patients – all of them – deserve better.
https://donoharmmedicine.org/wp-content/uploads/equality-equity.jpg627851Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2026-01-08 18:03:042026-02-11 15:34:18Michigan State Medical Society’s DEI Training: Ideology Masquerading as Medicine