Samantha Anderer’s Medical News in Brief, Thyroid Disease May be Overdiagnosed, Study Finds, recounted an articlein the Annals of Internal Medicine which found that variables, including race, may significantly influence thyroid hormone levels and affect diagnostic accuracy.[1],[2]
Compared to current laboratory reference values, the distribution of thyroid disease diagnosis greatly changed when accounting for race. According to the Annals article, 50.1% of whites diagnosed with subclinical hypothyroidism under current standards moved to the normal category once age-, sex-, and race-specific reference intervals were considered. For blacks, it was 14%. Moreover, for blacks, 60% moved from the subclinical hyperthyroidism to normal. The same was true for 17.3% of whites under an age-, sex-, and race-specific reference range.[3]
The authors concluded: “These findings should help establish more accurate reference intervals for thyroid disease […].”[4] If correct, then a change in parameters partly based on race would improve diagnostic precision, minimize unnecessary treatment, and lower avoidable healthcare costs.
This appeal to accuracy in diagnosis comes in contrast to the debate over estimated glomerular filtration rate (eGFR). In that setting a race correction was called “race-based medicine” given race’s “social construct.”[5]Yet, have we sacrificed clinical precision in pursuit of an illusory sense of equity?
It seems so. Proponents of a race-neutral equation claim that the race-corrected calculation underestimates renal disease severity in many black patients leading to delayed treatment. However, in his article, “Retaining Race in Chronic Kidney Disease Diagnosis and Treatment,” Paul Williams compares in great detail the race-corrected 2009 Chronic Kidney Disease Epidemiology Collaboration formula with the race-free 2021 version, showing that the 2009 formula better aligns with the true measure of GFR.[6]
Joel Velasco and Brad Snodgrass echoed this point in highlighting the harm to black patients by removing the race correction. They specifically noted the safe and effective prescribing and dosing of metformin necessitates an accurate eGFR.[7]Likewise, certain antibiotics, anticoagulants, and antihypertensives require a precise eGFR, not a political one. Even more critically, eGFR guides decisions on dialysis and transplant eligibility – making accuracy vital.
Delivering the highest quality care requires precision. While we have a moral obligation to treat people fairly, disregarding race when it can be clinically meaningful is misguided and can result in unequal treatment. May the same rigor being applied to thyroid diagnostics return to measures like eGFR, which were hastily politicized in the name of equity and at the expense of truth.
[1]Anderer S. Thyroid Disease May Be Overdiagnosed, Study Finds. JAMA. 2025;333(24):2134–2135. doi:10.1001/jama.2025.6466
[2] Qihang L, Yida T, Xuefeng Y, et al. Thyroid Function Reference Intervals by Age, Sex, and Race: A Cross-Sectional Study. Ann Intern Med. [Epub 6 May 2025]. doi:10.7326/ANNALS-24-01559
[3] Qihang L, Yida T, Xuefeng Y, et al. Thyroid Function Reference Intervals by Age, Sex, and Race: A Cross-Sectional Study. Ann Intern Med. [Epub 6 May 2025]. doi:10.7326/ANNALS-24-01559
[4]Qihang L, Yida T, Xuefeng Y, et al. Thyroid Function Reference Intervals by Age, Sex, and Race: A Cross-Sectional Study. Ann Intern Med. [Epub 6 May 2025]. doi:10.7326/ANNALS-24-01559
[5] Cerdeña JP, Plaisime MV, Tsai J. From race-based to race-conscious medicine: how anti-racist uprisings call us to act. The Lancet. 2020;396(10257):1125-1128
[6] Williams P. Retaining Race in Chronic Kidney Disease Diagnosis and Treatment. Cureus. 2023;15(9). doi: 10.7759/cureus.45054
[7]Velasco JD, Snodgrass B. The Use of Race in eGFR: Why Racial Justice Requires Accuracy. The American Journal of Medicine. 2021; 134(7):827-828
https://donoharmmedicine.org/wp-content/uploads/2024/11/shutterstock_2481473875-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-07-07 13:03:472026-02-11 15:34:08Refining Diagnostic Precision: The Impact of Race in Clinical Labs
The Centers for Medicare and Medicaid Services (CMS) is considering cutting off funding for children’s hospitals that provide sex change interventions to minors, The Wall Street Journal reported earlier this week.
The report comes on the heels of a CMSletter warning several children’s hospitals that child sex change interventions “lack reliable evidence of benefits.”
The letter gave the hospitals a 30-day deadline beginning May 28 to provide information and data related to their sex change services.
The hospitals include Children’s Hospital of Philadelphia, Seattle Children’s Hospital, Children’s Hospital Los Angeles, Boston Children’s Hospital, Children’s National Hospital, UCSF Benioff Children’s Hospital Oakland, Children’s Hospital Colorado, UPMC Children’s Hospital of Pittsburgh, and Cincinnati Children’s Hospital Medical Center, the WSJ reported.
These hospitals are ALL on Do No Harm’s “Dirty Dozen” list of the most prolific providers of child sex change interventions.
This list was created as part of Do No Harm’s Stop the Harm Database, a first-of-its-kind national database of hospitals and medical facilities administering irreversible sex change interventions on children in the United States.
Do No Harm has worked to shed light on these hospitals’ practices, profiling them and their gender activism. For instance, Do No Harm launcheda digital campaign targeting the Children’s Hospital of Philadelphia, highlighting the hospital’s devotion to gender ideology.
This is welcome scrutiny from CMS: Do No Harm supports efforts to ensure that taxpayer dollars are not used to support dangerous and experimental procedures to which children cannot consent.
The Do No Harm in Medicaid Act, sponsored by Representative Dan Crenshaw and endorsed by Do No Harm, would codify prohibitions on Medicaid funding for child sex change interventions.
Several of the hospitals have suspendedtheir sex change services in the wake of pressure from the Trump administration; Children’s Hospital of Los Angeles, citing the CMS letter, announced last month it would no longer provide so-called “gender-affirming care” to children.
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_361382480-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-07-02 13:45:292026-02-11 15:34:08CMS Could Cut Funding for Children’s Hospitals Performing Sex Change Interventions on Minors
Over the past few years, a movement has emergedto expand the scope of healthcare research and practice to “social determinants of health” (SDOH) – social, economic, and environmental conditions that can be construed as influencing individuals’ health.
Some commonly-cited examples of SDOH include income, employment, educational quality, housing quality, transportation, and so on.
Now, the authors of a commentarypublished in JAMA Surgery, titled “Quantifying Social Vulnerability and Its Impact on Health Care Delivery, Payment, and Performance,” argue that SDOH data should be integrated into patients’ electronic health records.
This means that SDOH data will likely inform individual care decisions by healthcare professionals.
The authors justify this position by arguing that SDOH “should dictate how we deliver the most appropriate care to each patient.”
They then go a step further, arguing that “[s]urgical research directed at health care delivery should consider these data in a similar way to the contributions of medical comorbidities.”
Yet the fundamental assumption behind the authors’ argument – that SDOH are the cause of disparities in health outcomes between populations, with the authors arguing that SDOH are “drivers of inequities” – is seriously flawed.
Although SDOH may be correlated with disparities in health outcomes, the evidence that SDOH cause poor health outcomes is shoddy and weak, at best.
Much of the scholarship on the topic confuses social and economic conditions that correlate with poor health outcomes with the actual causes of those outcomes, ignoring other factors such as individual agency and health decisions that contribute to health outcomes.
As Manhattan Institute Senior Fellow Chris Popelays out, “SDOH literature is dominated by sloppily designed observational studies that do not seriously attempt to disentangle causation from correlation or to control for obvious sources of bias.”
Citing Yale University economist Jonathan S. Feinstein, Pope notes that smoking, for example, is more common among poorer people and explains “much of the disparity in health outcomes.”
In other words, although income levels may be correlated with worse health outcomes, the cause of that disparity (in this example) is individual choice. Whereas the SDOH theory may attribute that disparity to poverty, the real culprit is not so easily pinned down.
As another example, a studypublished in The Quarterly Journal of Economics, examined the question of nutritional inequality: why do higher-income groups of people eat healthier than lower-income groups of people?
The study found that 90% of this “nutritional inequality” is driven by differences in demand; in other words, it was the choices of the lower-income people, not the environmental factors, that caused this disparity.
The “food desert” theory of nutritional inequality, which attributes the fact that lower-income people eat unhealthy foods to lack of supply of healthy food, had the causality backward.
To further illustrate the point that adjusting SDOH does not necessarily produce positive health outcomes, we can look at the results of anexperimentwith Universal Basic Income (UBI).
Under the SDOH theory, in which income levels determine people’s health outcomes, increasing income should improve health outcomes.
But when nineteen counties in Texas and Illinois tested out the UBI program, recipients “reported no increase in access to or utilization of health care,” UBI did not lead to lasting “physical or mental health improvements,” and “recipients were four percentage points more likely to report a disability or health problem that limits the work they can do.”
Advocates for the SDOH theory of health disparities are thus making the elementary mistake of confusing correlation with causation, or more pointedly, ignoring other causal and confounding factors that undermine the SDOH theory’s explanatory value.
This is not to say that SDOH cannot ever contribute to health inequities, but rather that evidence for SDOH as “drivers of inequities” is wanting, to say the least.
In a nutshell, “social determinants of health” don’t actually “determine” health.
In addition, many studies purporting to show the effects of SDOH on health outcomes fail to consider the effects of personal agency, such as patient’s health choices or adherence to health programs, when identifying health disparities that they attribute to SDOH.
For instance, one of the studiescited by the JAMA Surgery article identifies disparities in emergency gall bladder removals for individuals with higher social vulnerability scores compared to lower scores.
However, the study fails to make any mention of personal choices that may have impacted the need for the emergency procedure, such as decisions to seek care at earlier junctures. The social vulnerability index used in the study does include factors that could potentially impact these decisions, such as distance to the hospital, but does not disaggregate the actual healthcare choices made by the patients from its analysis.
This omission implicitly assumes the causal effect of SDOH without considering the confounding variables that may be correlated with SDOH.
And finally, there is the authors’ position that “[s]urgical research directed at health care delivery should consider these data in a similar way to the contributions of medical comorbidities.”
One of the problems with this position, beyond the causal issues identified earlier, is the lack of a limiting principle; should surgical research consider everything?
SDOH, by their very nature, describe just about every conceivable factor in an individual’s environment that could be construed as affecting an individual’s health. The universe of possibilities is endless.
The resulting policy implications are likewise too broad and removed from the focus of healthcare. Put simply, it is not the role of medical professionals to become transit activists or education reformers.
Such activities are beyond the purview of medicine, and this mission creep comes at the detriment of medicine’s core focus.
https://donoharmmedicine.org/wp-content/uploads/2025/07/shutterstock_2509717171-scaled.jpg17032560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-07-01 14:10:552026-02-11 15:34:08The Flawed Logic Behind the ‘Social Determinants of Health’ Theory of Medicine
In January 2025, West Virginia Governor Patrick Morrissey signed an executive order restricting DEI initiatives at state-funded entities, such as West Virginia University (WVU).
The order, among other things, prohibits state-funded entities from “grant[ing] preferential treatment based on one person’s particular race, color, sex, ethnicity, or national origin over that of another.”
In response to the executive order, WVU shuttered its DEI department, according to a response to a public records request submitted by Do No Harm. The school’s Vice President for Diversity, Equity, and Inclusion was earning $239,372.00 per year, the records showed.
However, WVU’s School of Medicine still advertises a number of DEI initiatives and commitments on its website.
For instance, the WVU Department of Ophthalmology and Visual Sciences still advertises its commitments to diversity, including language that appears to gesture at granting preferential treatment to individuals of certain backgrounds.
“Our goal is to recruit faculty and trainees of different backgrounds to better serve our patients, foster a learning environment that celebrates individuals of all backgrounds, and train culturally competent physicians who will thrive in any setting they find themselves in after graduation,” the department’s “Diversity, Equity, and Inclusion” webpage reads.
“We have recently initiated a program of scholarships to students at medical schools in historically black colleges and universities who choose to perform clinical or research rotations in ophthalmology at WVU,” the webpage continues; it’s not clear exactly what program the webpage refers to.
Similarly, the WVU Department of Otolaryngology mentions its efforts to increase diversity within its residency program on its “Diversity” webpage.
“We strive to recruit residents and faculty from minoritized communities who are traditionally underrepresented in medicine,” the webpage states. “We additionally greatly value individuals from all backgrounds including those from economically and educationally underserved communities.”
The page goes on to refer to the department’s “Diversity/Pipeline Programs and Partnerships.”
“Our health science center engages in ongoing and focused recruitment and retention activities to aid us in achieving diversity amongst our trainees, faculty and staff. This includes programs and/or partnerships between key Diversity, Equity, and Inclusion focused personnel, and our Otolaryngology Residency.”
WVU’s School of Public Health likewise maintains its webpagelisting the “diversity initiatives,” though much of that information appears to be out-of-date.
These initiatives include links to DEI trainings, as well as webpagetitled “Racism is a Public Health Crisis.”
That webpage provides a list of organizations with whom students can “get involved,” including Color of Change, the NAACP, the Equal Justice Initiative, the Black Student Union at West Virginia University, and Call to Action for Racial Equality (CARE) West Virginia.
WVU should end all of its divisive and discriminatory programming – for good.
https://donoharmmedicine.org/wp-content/uploads/2023/09/shutterstock_124304896-scaled.jpg15362560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-06-30 21:10:302026-02-11 15:34:08Despite Executive Order, West Virginia University Medical School Advertises DEI Programs
It appears the American Society of Anesthesiologists (ASA) is numb to the real interests of its members.
The ASA sent out a survey, obtained by Do No Harm, asking its members to share their opinions on a series of prompts related to DEI and DEI trainings.
It’s not clear how this information is relevant or helpful to an organization representing anesthesiologists, but according to the survey, the ASA plans to use it to inform its DEI trainings and educational offerings.
First, the survey prompts readers with misleading and favorable definitions of diversity, equity, and inclusion.
In particular, the survey states that “equity” ensures “that everyone has access to similar opportunities,” and that “inclusion” ensures that all individuals “have equal access to opportunities, resources, and participation in all aspects of society, organizations, or communities.”
Figure 1. A screenshot from the ASA survey,
In practice, however, DEI does the exact opposite: it restricts access to opportunities on the basis of race, doing so in the name of achieving “equity” and “diversity.”
Later in the survey, the ASA asks members to answer how important it is for health professionals to receive DEI competency training.
Figure 2. A screenshot from the ASA survey.
Next, the ASA asks members specifically how much training they have received on DEI at various stages of their educational journey.
Figure 3. A screenshot from the ASA survey.
And finally, the ASA asks its members to answer whether they believe they’ve received “enough” DEI training.
Figure 4. A screenshot from the ASA survey.
The ASA’s DEI-related activities provide some clues on how the organization plans to use this information; on its website, the ASA lists a host of diversity resources and statements in support of DEI.
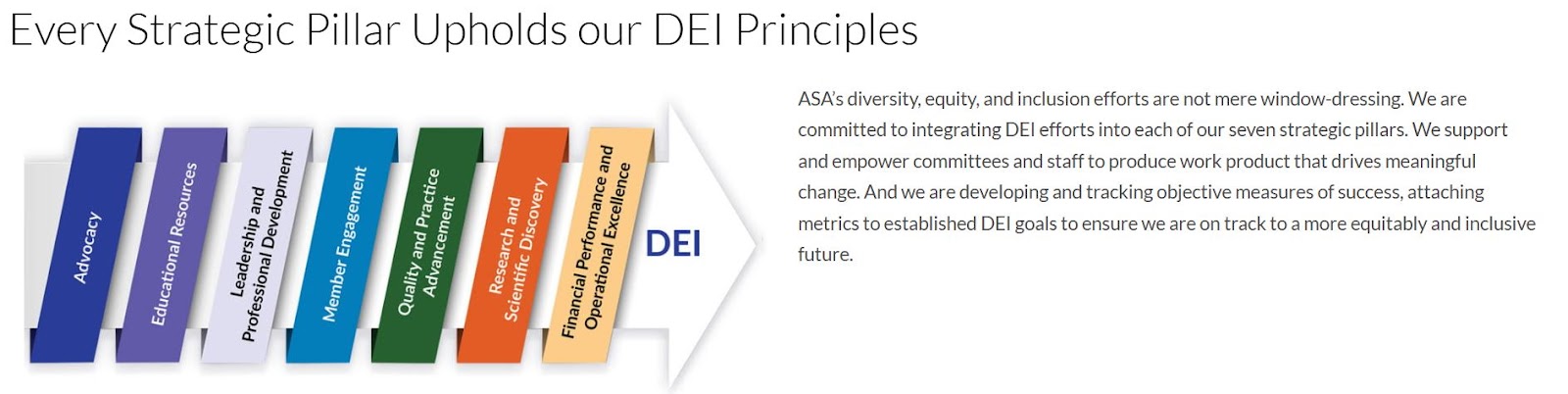
For instance, the ASA maintains a graphic on its website explaining how each “Strategic Pillar” upholds the organization’s DEI principles.
“ASA’s diversity, equity, and inclusion efforts are not mere window-dressing. We are committed to integrating DEI efforts into each of our seven strategic pillars,” an ASA statement accompanying the graphic reads. “We support and empower committees and staff to produce work product that drives meaningful change. And we are developing and tracking objective measures of success, attaching metrics to established DEI goals to ensure we are on track to a more equitably and inclusive future.”
Figure 5. A screenshot of the ASA’s “Strategic Pillars” demonstrating the organization’s commitment to DEI.
The ASA’s DEI page also links to a lecturetitled “Anesthesiology must lead in diversity, equity, and inclusion.”
In other areas of the website, the ASA’s commitment to DEI is also on full display.
For instance, the organization advertisesits DEI principles on its web page promoting careers within ASA.
“We are committed to increasing the representation of individuals from groups underrepresented in anesthesiology and ensuring that future Anesthesiologists have the tools to care for patients from diverse backgrounds,” the ASA Medical Student Component’s diversity statementreads.
The website also contains a DEI lecture series, including an interview with an anesthesiologist at the University of Chicago who discussed “the importance of the social determinants of health and his efforts to create a more diverse and inclusive workforce.”
The ASA, like many other medical associations, appears more concerned with imposing a divisive and discriminatory ideology onto its members than furthering the interests of the medical field.
https://donoharmmedicine.org/wp-content/uploads/2025/06/shutterstock_2467819873-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-06-27 15:21:172026-02-11 15:34:08American Society of Anesthesiologists Grills Members on Support for DEI
Back in March, Do No Harm releaseda report highlighting how accreditors’ power over institutions of higher education, particularly in medical education, enables them to inject political agendas into universities’ policies.
Now, there’s a sign that accreditors’ stranglehold on public education may be breaking.
Six public university systems announced plans Thursday to launch a new accrediting agency for public higher education institutions.
The University of Florida System, University of Georgia System, University of Tennessee System, University of North Carolina System, University of South Carolina System, and Texas A&M System together announced the creation of the Commission for Public Higher Education in a press release. The commission will develop an accreditation model aimed at prioritizing “academic excellence, student outcomes and achievement.”
The press release describes the new body as a “consortium of higher education systems from several states offering a new accreditation model that will focus on academic excellence, student outcomes, process efficiency, and the pursuit of quality assurance for public postsecondary education.”
“By establishing rigorous, transparent, and adaptable outcomes-based accreditation standards and practices, CPHE will ensure that colleges and universities meet and maintain academic quality and operational excellence on behalf of their students,” the press release states.
New accreditation models are sorely needed in medical education: as Do No Harm reported, accreditors often use their perches to require universities and medical schools to engage in divisive and discriminatory policies
This problem prompted President Trump to issue an executive ordertargeting accreditors for their ideological mandates.
Although the two main medical education accreditors, the Accreditation Council for Graduate Medical Education (ACGME) and the Liaison Committee on Medical Education (LCME), have since walked back their DEI standards, many others have not.
An alternative accreditation model enables universities to operate without deferring to the whims of the entrenched accreditors.
Do No Harm supports all attempts to direct medical education toward the values of excellence, achievement, and merit.
https://donoharmmedicine.org/wp-content/uploads/2022/05/shutterstock_59868724-scaled.jpg17052560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-06-27 15:06:102026-02-11 15:34:08University Systems Announce Alternative Accreditation Model Prioritizing ‘Academic Excellence’
This past May I had the opportunity to attend the American Psychiatric Association (APA) annual meeting in Los Angeles along with Ian Kingsbury, Do No Harm Director of Research, and Dr. Miriam Grossman, Do No Harm Senior Fellow. It was the first time I came as an exhibitor, and it has been at least a decade since I’ve been a full program attendee. I entered as part of Do No Harm, and to hear – for what I believe was the first time – general sessions on both sides of the debate surrounding the care of minors with gender dysphoria.
Serious concerns surrounding the evidence for pediatric medical transition – puberty blockers, cross-sex hormones, and surgeries – are not unique. Systematic reviews reveal the very low quality of evidence for any beneficial effects compared to the risk of significant, irreversible harms. Even the World Professional Association for Transgender Health (WPATH) itself noted in its Standards of Care for the Health of Transgender and Gender Diverse People, Version 8 (SOC-8) that a “key challenge in adolescent transgender care is the quality of evidence evaluating the effectiveness.” It goes on to state that “adolescents, their parents, and care providers should be informed about the nature of the evidence base.”
Yet, WPATH has not heeded its own warning, leading professional medical associations to unfortunately place the cart before the horse in issuing guidance before appropriately assessing the evidence. Prior to understanding or performing systematic reviews, many organizations within the medical establishment made their policy position known. The American Academy of Pediatrics (AAP), for example, issued aPolicy Statement in 2018, which it later reaffirmed in 2023, fully supporting an “affirming” model, and nothing else. And while the AAP called for a “systematic review of the evidence” in 2023, none has yet to be delivered.
The same goes for the American Psychiatric Association, whose Assembly and Board of Trustees approved aPosition Statement in 2020 supporting “access to affirming and supportive treatment for trans and gender diverse youth and their families, including appropriate mental health services, and when indicated puberty suppression and medical transition support.” An affirming model was fully and solely endorsed; reference to “mental health and social support services” was merely mentioned in the context of “navigat[ing] the gender affirmation process.”
The Europeans followed a different course than our U.S.-based medical societies. Finland, Sweden, and the United Kingdomissued systematic reviews to inform their analysis. Their work highlighted the low quality of evidence for an affirming model that includes puberty blockers, hormones, and surgeries for children and adolescents with gender dysphoria. They found a lack of evidence supporting the safety and efficacy of these treatments in minors. Caution was strongly advised and these otherwise experimental medical and surgical interventions were sharply restricted. Clear priority was given to psychosocial support and psychotherapy.
Despite the evidence from overseas, many U.S. medical organizations maintain a pro-affirmation stance and have historically silenced debate in the face of any disagreement. However, the 2025 APA annual meeting showed signs of change. For one, Do No Harm’s exhibit allowed for meaningful one-on-one conversations with many attendees. We spoke with those caring for youth with gender dysphoria as well as students just learning about this condition. Our discourse was free and open. I’m encouraged to think these same open-minded individuals will also give a fair reading to the Department of Health and Human Services’ report on this topic.
Moreover, the APA talks on the subject were highly informative, and perhaps for some, eye-opening especially when juxtaposed with one another. One session in particular looked at the data from Europe and the role of systematic reviews. Drs. Christian Monsalve, Stephen Levine, Kristopher Kaliebe, and Kathleen McDeavitt did a phenomenal job in clearly and professionally reviewing the evidence. Credit goes to these outstanding speakers as well as Dr. Michael Myers, Chair of the Scientific Program Committee, for making this happen.
I also applaud the persistence of those who have been petitioning the APA for this conversation. I understand these efforts to raise serious and legitimate concerns regarding pediatric medical transition have been a long time coming to a national meeting like the one I recently attended. For years, dissenting views within the medical community that challenged the prevailing narrative around so-called “gender-affirming care” were effectively muted. May this silencing finally have come to an end.
Indeed, the moment has arrived for the APA – and other specialty medical societies – to demonstrate responsible leadership and change course from the past. Duty to the members of these associations, the integrity of medical practice, and, most importantly, the patients themselves, demands an open and rigorous examination of the evidence. Systematic reviews cannot be ignored. Neither can the serious risks associated with the current affirming model. Frankly, this exercise should have transpired within organized medicine well in advance of one-sided policy statements, which unfortunately have been informed more by politics than solid evidence.
In this regard, debate must occur in an honest and transparent manner throughout the halls of medicine. Medical societies should not fear the public, but welcome their desire for knowledge. If medical societies like the APA seek to earn the public’s trust at this point in the debate, then these medical associations need to dialogue openly and truthfully.
While the press was, unfortunately, not permitted at these sessions of the APA, this practice must end. The closed doors must be opened. Silence gives the sense of a false unanimity that only so-called “gender-affirming care” is supported by the medical community, when in fact there are many physicians with grave concerns about the harms these interventions have on youth.
Today we are at a critical moment. A careful review of the HHS report is essential. As an umbrella review, seventeen systematic reviews met the report’s inclusion criteria. And, as with the various European analyses, the conclusion was clear: The overall quality of evidence regarding the psychological, quality of life, and long-term health effects of pediatric medical transition is very low. In other words, the reported benefits of these interventions are likely to be significantly different from actual outcomes.
The evidence also indicates these interventions are not lifesaving. Yet, some physicians advocating for pediatric medical transition pressure anxious parents by citing an alleged increased risk of suicide, a claim that is both unfounded and unethical, as noted in the HHS report. Likewise, serious, irreversible risks of these interventions must not be overlooked, including infertility, sexual dysfunction, impaired bone mineral density, cardiovascular ailments, surgical complications, and regret, the latter of which the true rate is simply not known.
More so, the role of physician extends beyond mere technical expertise. Doctors have a duty to thoughtfully consider a minor’s inability to consent or assent to treatment and the ethical implications of their clinical recommendations in light of this reality. The Boe v. Marshall case underscored this concern, as the Johns Hopkins University team, which was contracted by WPATH as part of SOC-8, found insufficient evidence to support the claim that adolescents possess the capacity to consent to these interventions. Furthermore, when considering issues like fertility, we must recognize that an adolescent’s limited life experience places significant limitations on his or her ability to truly comprehend future desires.
From an ethical standpoint, it is also important to recognize that patients do not have an inherent right to medications and procedures that lack demonstrable benefit. Autonomy, while valued, is not the sole guiding ethical principle in medical decision-making. Physicians must also remember both beneficence and nonmaleficence, ensuring that their recommendations prioritize the patient’s well-being and safeguard against harm. Physicians must move beyond “have it your way” medicine and remember they’re not working for Burger King but rather caring for people. May that sacred duty never be forgotten.
Psychiatrists, too, must not abandon the essential role they play in the care of minors with gender dysphoria. The vast majority of these children have co-occurring psychiatric conditions or have experienced significant trauma – factors that warrant careful evaluation and treatment. In fact, high-quality psychotherapy first requires a comprehensive understanding of the underlying and sustaining factors contributing to a patient’s distress. Subsequently, psychotherapeutic approaches such as cognitive behavioral therapy, dialectical behavioral therapy, psychodynamic psychotherapy, and family therapy, among others, can offer meaningful impact. Clearly, these non-invasive options should serve as an obvious first-line treatment.
The APA’s recent meeting marks progress toward open discourse and more ethical practice. While past policy statements have been issued without comprehensive systematic reviews, the willingness to engage in debate signals a shift toward greater intellectual rigor. However, much more is needed from medical associations, specifically policies and guidelines grounded in science and the evidence base. Ultimately, the APA – and other specialty societies – must revisit their own position statements on pediatric medical transition. An update is sorely needed given the data before us. Ending pediatric medical transition and moving toward genuine psychosocial support and psychotherapy is essential to prioritizing the long-term health and well-being of children suffering from gender dysphoria.
https://donoharmmedicine.org/wp-content/uploads/2024/07/shutterstock_2342854455-scaled.jpg14402560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-06-26 12:44:352026-02-11 15:34:08Evidence Over Politics: Rethinking Gender Medicine in Psychiatry and Beyond
According to a letter obtained by Do No Harm, the Southern California Society of Child and Adolescent Psychiatry (SCSAP) decided to offer its members a “Fellows Grant” to cover the costs of attending the 2025 Annual Meeting of the American Academy of Child and Adolescent Psychiatry (AACAP).
The grant includes up to $750, and is available to active SCSAP members.
Yet the SCSAP seems to have particular racial groups in mind for the grant.
According to the letter, “[f]ellows who meet the AAMC URiM definition below and those with an interest in justice, equity, diversity and inclusion (JEDI) are encouraged to apply.”
The letter goes on to then reference the Association of American Medical Colleges’ definition of “underrepresented in medicine,” which has since been removedfrom the AAMC website.
“The AAMC defines underrepresented in medicine (URiM) groups as ‘racial and ethnic populations that are underrepresented in the medical profession relative to their numbers in the general population,’” the letter reads.
“Individuals from underrepresented minority (URM) groups, ‘which consists of Black, Mexican-American, Native Americans [sic] (that is, American Indians, Alaska Natives, and Native Hawaiians), and mainland Puerto Ricans [sic]’ are particularly encouraged to apply.”
Additionally, applicants must answer the following two questions: “Why is justice, equity, diversity and inclusion important to you?”; and “What do you hope to gain or experience from the 2025 AACAP meeting in Chicago?”
This initiative reflects a disturbing trend in medicine, where access to opportunities is increasingly defined by racial background and adherence to ideology rather than merit.
By prioritizing certain racial or ethnic groups and tying funding to a commitment to “justice, equity, diversity and inclusion,” the SCSAP sends a message that immutable characteristics matter more than ability.
https://donoharmmedicine.org/wp-content/uploads/2025/05/shutterstock_2533816059-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-06-25 20:36:002026-02-11 15:34:08Psych Association Targets Specific Racial Groups for ‘Fellows’ Grants
Last night, the FBI launched criminal investigations targeting three children’s hospitals on Do No Harm’s list of top offenders.
The probes follow on the heels of a memo by Attorney General Pam Bondi directing the Department of Justice to enforce a federal statute that prohibiting female genital mutilation.
Additionally, President Trump issued executive orders protecting Americans from the unconscionable ideology behind so-called “gender-affirming care.”
These probes represent aggressive action – backed by federal authority – to further protect children from irreversible and experimental procedures. They specificallytarget Boston Children’s Hospital (BCH), Children’s Hospital Colorado (CHC), and Children’s Hospital Los Angeles (CHLA); all hospital’s on Do No Harm’s “Dirty Dozen” list of the most prolific providers of child sex change interventions.
Last October, Do No Harm released the Stop the Harm Database, a first-of-its-kind national database of hospitals and medical facilities administering irreversible sex change interventions on children in the United States. Just scratching the surface, the database exposed key findings about these three hospitals.
By the Numbers (BCH, CHC, and CHLA from 2019 to 2023):
686 Total sex change patients
337 Total surgery patients
360 Total hormone and puberty blocker patients
2,500 Total prescriptions written
$8,474,775 Total submitted charges
Additionally, Attorney General Pam Bondi will soon launch a new taskforce, the Coalition Against Child Mutilation, joining forces with state attorneys general across the country to hold hospitals and practitioners that violate laws against female genital mutilation accountable.
Part of this development includes an effort to establish a private right of action for children and parents of children “whose healthy body parts have been damaged by medical professionals through chemical and surgical castration.”
This is a massive victory, and there’s more to come. The days of children being subjected to dangerous, irreversible procedures are numbered.
https://donoharmmedicine.org/wp-content/uploads/2024/08/shutterstock_1950794986-scaled.jpg17342560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-06-25 20:30:552026-02-11 15:34:07FBI Launches Probes Into Children’s Hospitals That Performed Child Sex Change Interventions
One would think that, as more and more Americans realizethe harms associated with DEI, medical associations would read the room and ditch their commitments to this ideology.
Not so at the American College of Academic Addiction Medicine (ACAAM).
In April 2025, the ACAAM Board of Directors “reconfirmed the organization’s commitment to the following actions, which are based on advancing Diversity, Equity, and Inclusion (DEI) in all the organization does,” the organization announced in a statement.
These actions include: “Commit to ongoing efforts to embrace diversity within the organization and act to promote an inclusive and equitable environment among the addiction medicine workforce”; “Maintain educational resources related to anti-racism, cultural competence, social disparities of health & social justice […]”; and “Recruit and train students, residents, fellows and addiction specialists from minoritized populations in the addiction medicine workforce and pathways.”
The last item in particular, depending on how the ACAAM aims to achieve it, appears to imply that the ACAAM will engage in racial discrimination.
Additionally, on its website, the ACAAM promotes a host of resources aimed at promoting DEI in the substance use field.
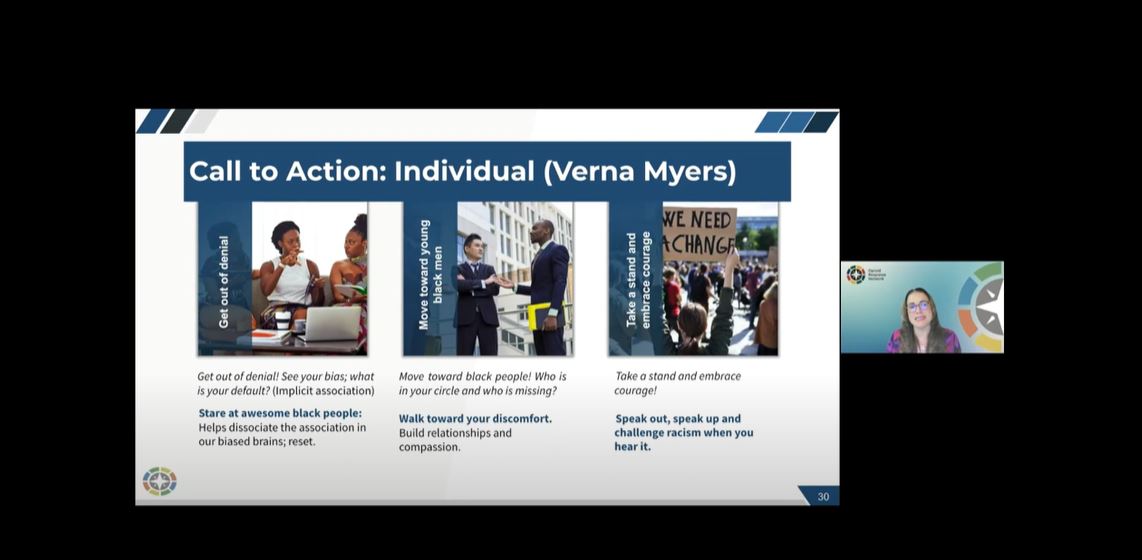
This includes the “Advancing Racial Equity in the Substance Use Field” presentation, a “two-part pre-recorded racial equity training series focused on the substance use field.”
One of the recommended behaviors in the presentation’s call to action was to “stare at awesome black people.”
Yes, really.
Another segment of the presentation stated that as part of “anti-racist” leadership, organizations should “promote and elevate BIPOC employees” and “recruit and hire staff to reflect the client population.”
Figure 1. A screenshot from the “Advancing Racial Equity in the Substance Use Field” presentation.
Other presentations included “Academic Addiction Medicine Responds: Addressing Racism, Diversity, Equity, and Inclusion” and “Unpacking Racial Disparities in Addiction and a Path Forward.”
Moreover, one presentationtitled “Identifying and Addressing Implicit Bias in Our Work” featured an article arguing that “medicine is not a stand-alone institution immune to racial inequities, but rather is an institution of structural racism.”
In sum, these resources demonstrate the ACAAM’s deep institutional commitment to DEI.
Healthcare professionals should be guided by merit and excellence, not ideology.
https://donoharmmedicine.org/wp-content/uploads/2025/06/shutterstock_2457309399-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-06-23 14:51:022026-02-11 15:34:07The ACAAM Is Still Addicted to DEI
Emergency Medicine Reviews and Perspectives (EM:RAP) is a medical education program that provides instructional emergency medicine content and discussions through podcasts and videos.
The program bills itself as “the most listened to audio program in emergency medicine, with more listeners than the total number of emergency physicians in the United States.”
During a July 2024 episode of the EM:RAP podcast, several emergency medicine practitioners discussed so-called “anti-DEI” legislation and offered their support of DEI efforts.
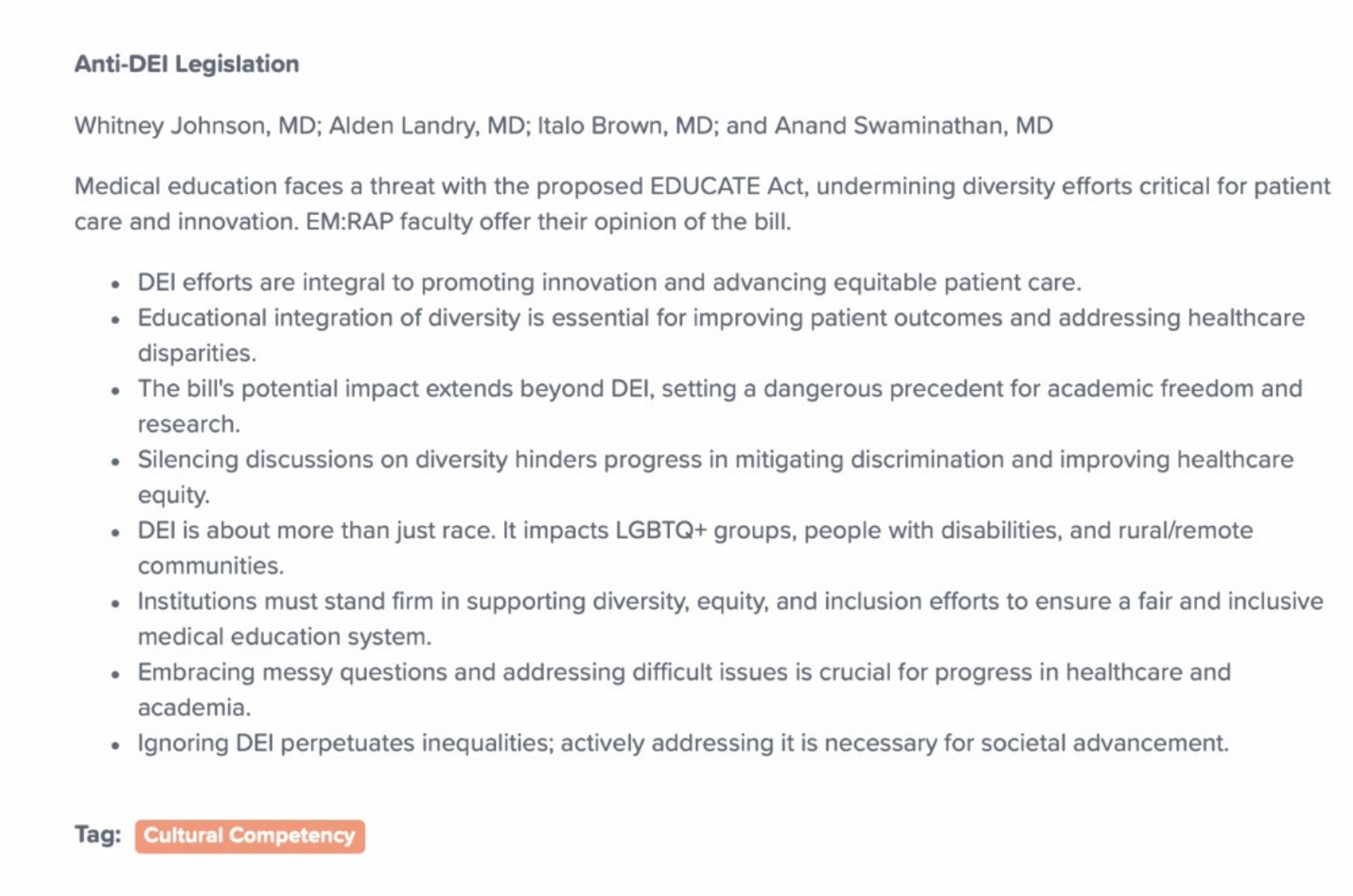
The focal point of the discussion was the EDUCATE Act, a bill introduced by Representative Greg Murphy (and recently reintroduced this spring) and endorsed by Do No Harm that would cut off federal funding to medical schools’ diversity, equity, and inclusion (DEI) programs.
The bill would defund programs that compel students or faculty to engage in racial discrimination, as well as block funding to medical schools that have DEI departments or functionally equivalent offices. The bill would also require accreditation agencies to remove DEI requirements while allowing instruction about ethnicity-related health issues.
Figure 1. A screenshot of the EM:RAP podcast episode summary.
The EM:RAP discussion featured faculty members, including Tiffany Mitchell, MD, Italo Brown, MD, and Alden Landry, MD. Predictably, the faculty members, who work at Mount Sinai, Stanford, and Beth Israel Deaconess hospitals respectively, opposed the bill, according to an episode summary that included various statements in opposition to the legislation and in support of DEI.
These statements included: “DEI efforts are integral to promoting innovation and advancing equitable patient care”; “Silencing discussions on diversity hinders progress in mitigating discrimination and improving healthcare equity”; and “Institutions must stand firm in supporting diversity, equity, and inclusion efforts to ensure a fair and inclusive medical education system.”
During the episode itself, the first guest to address the legislation, Dr. Brown, erroneously argued that it would exclude physicians of certain backgrounds.
“This felt like … people who took the same oaths that I took … had automatically decided that people who come from diverse backgrounds no longer should be considered to be in our brotherhood/fraternity/family of physicians,” Brown said.
The idea that legislation intended to restrict discriminatory practices is itself discriminatory is obviously wrong; the EDUCATE Act does not prevent individuals of certain backgrounds from becoming physicians. In fact, it does the exact opposite.
But Brown continued, arguing that the proper response to the EDUCATE ACT should be even more DEI advocacy on the part of the medical community.
“This is why advocacy, now more than ever, just needs to come from us. That we need to rise with all of our physician voices,” Brown said.
But the endorsements of DEI didn’t end there.
Later in the episode, Dr. Landry discussed the role of DEI offices in medical schools, arguing that DEI must be present in every corner of medical school administrations.
“I do think that every office of student affairs on a medical school campus should champion DEI offices,” he said. “Every DEI office of faculty affairs should champion DEI efforts. I think every office of research should champion DEI efforts … it should be in every office in every institution.”
The discussion concluded with an endorsement of DEI advocacy from Dr. Mitchell, who succinctly summed up the EM:RAP faculty’s position.
“All of our institutions, all of our hospitals, and schools, and courthouses should be proud to proclaim a commitment to diversity, equity, and inclusion. Full stop.”
EM:RAP is woefully out of touch with the reality of DEI, and its faculty appear to misunderstand the subjects they are discussing.
DEI, by its nature, divides individuals on the basis of race and encourages racial discrimination to achieve “equitable” ends.
Not only is DEI dangerous, it is antithetical to the ethical practice of medicine.
https://donoharmmedicine.org/wp-content/uploads/2024/06/shutterstock_1189798267-scaled.jpg14402560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-06-20 14:39:092026-02-11 15:34:07Emergency Medicine’s ‘Most Listened To’ Program Devolves Into DEI Activism
The Association for Applied Sport Psychology (AASP), initially intended to host its annual conferencefor 2026 in Orlando, Florida.
But in 2023, the organization elected to move its conference out of the Sunshine State and to Minnesota instead.
Why?
Because, according to a November 2023email from AASP leadership to the organization’s members, Florida’s laws restricting DEI and racial discrimination conflicted with AASP values.
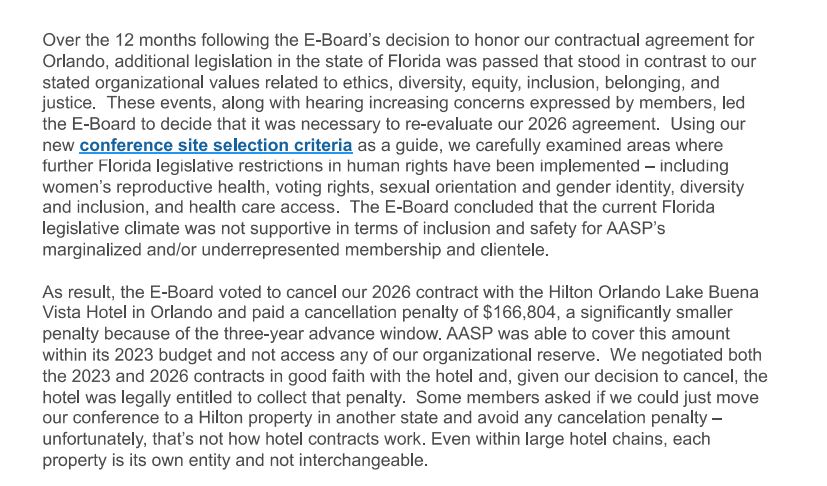
“Over the 12 months following the E-Board’s decision to honor our contractual agreement for Orlando, additional legislation in the State of Florida was passed that stood in contrast to our stated organizational values related to ethics, diversity, equity, inclusion, belonging, and justice,” the email read.
“These events, along with hearing increasing concerns expressed by members, led the E-Board to decide it was necessary to re-evaluate our 2026 agreement,” the email continued.
Figure 1. A screenshot of the AASP’s email announcing it would move its conference out of Florida.
The email then stated that the AASP paid a cancellation penalty of a whopping $166,804 to do so!
That doesn’t sound like money well spent. Instead of supporting programs and educational initiatives to advance the field of sports psychology, those funds are instead spent signalling the AASP’s commitment to divisive and discriminatory ideology.
Figure 2. A screenshot of the AASP’s email announcing it would move its conference out of Florida.
Additionally, the AASP email stated that the AASP “will not return” to Florida “until the legislative climate is more supportive of inclusion and safety of our members and the state becomes more welcoming to all.”
As for its existing institutional commitments to DEI, the AASP maintains a diversity statement on its website.
Moreover, it operates several diversity-focused programs and groups, including a Diversity Committee and a Diversity & Inclusion Council.
These actions demonstrate the AASP is, very literally, putting DEI ideology over the interests of its members.
A professional association subverting the interests of the members that the organization claims to represent is antithetical to core, foundational ethical principles.
https://donoharmmedicine.org/wp-content/uploads/2024/05/shutterstock_2288740175-scaled.jpg13502560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-06-19 12:12:002026-02-11 15:34:07Psychological Association Pays the DEI Tax to Move Conference Out of Florida
Today, the Supreme Court upheld a Tennessee law banning child sex change interventions including puberty blockers, cross-sex hormones, and surgical procedures.
Specifically, the Court held that Tennessee’s law is constitutional and does not discriminate based on sex or transgender status. This means that laws like Tennessee’s are legitimate and lawful, opening the door for other states to enact similar protections for children.
“Today the Supreme Court ruled, 6-3, that governments can enact commonsense policies that protect children from dangerous medical procedures,” said Stanley Goldfarb, MD, Chairman of Do No Harm. “The decision should end the debate over laws like Tennessee’s, and it could have important ramifications for other commonsense policies that resist radical gender ideology.”
“The Supreme Court’s strong decision today is a massive win in the fight to protect children from harmful gender ideology. Transgender treatments for minors are experimental medicine not backed by reliable evidence,” said Kristina Rasmussen, Executive Director, Do No Harm. “Do No Harm is proud to have been in the fight to expose this ideology over the last several years and support Tennessee in this case. We will continue to work nationally and in other states to protect children from the harms of sex change treatments.”
Tennessee’s law bans procedures enabling “a minor to identify with, or live as, a purported identity inconsistent with the minor’s sex” or to address “purported discomfort or distress from a discordance between the minor’s sex and asserted identity.”
The law reflects the fact that child sex change interventions are dangerous, carry unknown long-term risks, and are supported by weak, dubious, and error-filled evidence.
However, in April 2023, the ACLU, Lambda Legal, and Akin Gump Strauss Hauer & Feld LLP sued Tennessee to block enforcement of SB 1, arguing that the law violates the Equal Protection and Due Process Clauses of the Fourteenth Amendment, as well as Section 1557 of the Affordable Care Act.
That same month, the Department of Justice intervened in the case and filed its own complaint against Tennessee, also arguingthat the law violates the Fourteenth Amendment’s Equal Protection Clause.
The core of the plaintiffs’ argument is that Tennessee’s law discriminates on the basis of sex.
Laws that discriminate based on sex are subject to “intermediate scrutiny,” a heightened standard of review that requires states to demonstrate that the laws further an important government interest – and do so by means that are substantially related to that interest.
This standard of review is substantially more difficult to meet.
The Court held that Tennessee’s law did not discriminate on the basis of sex, nor did it discriminate on the basis of transgender status.
This is a massive victory for children in Tennessee and across the country. By upholding Tennessee’s law, the Court has provided a green light for states to enact laws protecting minors from harmful sex change procedures.
The Court’s ruling could potentially embolden more states to enact restrictions on these interventions, or encourage states with existing restrictions to strengthen their protections. Additionally, this ruling is a major blow to gender ideologues and activists intent on pushing sex change interventions on children.
The Court’s ruling that bans on child sex change interventions do not discriminate on the basis of sex could undermine future constitutional challenges to similar laws.
https://donoharmmedicine.org/wp-content/uploads/2023/09/shutterstock_78346810-scaled.jpg16952560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-06-18 17:10:352026-02-11 15:34:07A Massive Victory for Children Everywhere: The Supreme Court Upholds Tennessee Law Restricting Child Sex Change Interventions
https://donoharmmedicine.org/wp-content/uploads/2025/06/book_promo_v02_1280x720.jpg7201280dnhprodhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngdnhprod2025-06-17 19:38:162026-01-20 14:48:01Doing Great Harm?: How DEI and Identity Politics Are Infecting American Healthcare―and How We Are Fighting Back
In December 2024, Do No Harm released a comprehensive report exposing the Association of American Medical Colleges (AAMC) for injecting DEI into medical education. The report provides an in-depth examination of the AAMC’s DEI policies, advocacy, and agenda, identifying various resources either on the AAMC website or linked to the AAMC that promote “diversity” initiatives.
Following our report, President Trump issued an executive ordertackling DEI in the private sector and enforcing compliance with the Supreme Court’s ruling that race-based university admissions are illegal.
The executive order explicitly mentions “medical associations” and “institutions of higher education” with endowments over $1 billion, thereby covering many of the most prolific advocates of DEI and racial discrimination in the medical field.
In the months since our report was published, the AAMC has taken steps to remove dozens of the more explicit and overt endorsements of DEI from its website. These include resources on the AAMC’s own DEI programs, such as grant programs and training modules, as well as commitments to diversity in medical school admissions and hiring/recruiting.
However, these steps have largely been cosmetic; many of the AAMC’s DEI resources remain, and webpages are still active for DEI programs, including ones that discriminate on the basis of race.
Additionally, the AAMC has yet to distance itself from its long history of DEI activism and its promotion of racial discrimination in its public statements.
One example of the AAMC scrubbing or altering resources is the AAMC’s webpage on “Diversity in Medical School Admissions.”
The page, among other things, included links to resources critical of the Supreme Court’s ruling in Students for Fair Admissions v. Harvard, which found race-conscious admissions to be unconstitutional, as well as various statements expounding on the value of racial diversity in medical admissions.
“Diversity, equity, and inclusion (DEI) in medical education and the physician workforce is critical for everyone’s health,” the page stated. “Incorporating DEI programs into medical education is about helping future doctors better understand the specific issues that each patient is facing to provide better medical care.”
That page now redirects to a webpage titled “Equal Opportunity in Medical School Admissions.”
That webpage includes a statement explaining the AAMC’s position regarding compliance with the Supreme Court’s ruling.
“A workforce or classroom benefiting from a diversity of experiences and backgrounds continues to be a worthwhile goal, but pursuit of that goal must be fair and free from any unlawful discrimination,” the statement says.
Additionally, the AAMC removeda general resource page dedicated to the AAMC’s various DEI initiatives, statements, and programs.
That page, as evidenced in the screenshots below, included links to recent AAMC activity on the DEI front and new resources regarding equity, diversity, and race.
Figure 1. A screenshot of the AAMC’s former “Equity, Diversity, and Inclusion” webpage.Figure 2. A screenshot of the webpage for the AAMC’s “Equity, Diversity, and Inclusion Initiatives.”
The webpage for one of the resources, “Equity, Diversity, & Inclusion Initiatives” now redirects to a webpagetitled “Initiatives to Cultivate Excellence in Academic Medicine.”
Several of the “initiatives” included in both lists are effectively the same programs, but in the latter list the more offensive programs have been largely rebranded to remove overt DEI language or removed altogether.
For instance, as mentioned previously, the “Diversity in Medical School Admissions” initiative page is now the “Equal Opportunity in Medical School Admissions” initiative page. Both pages contain a list of resources related to the Supreme Court’s SFFA decision, but resources more overtly related to DEI are absent from the latest version.
As another example, the AAMC’s webpage for its IDEAS education series remains active. IDEAS stands for “Inclusion, Diversity, Equity, [and] Anti-racism” and features presentations and courses intended to advance DEI in medicine. According to a previous versionof the IDEAS homepage, “improving inclusion, diversity, equity, and anti-racism is a critical priority for the academic medicine community.” That language is no longer present.
The AAMC’s webpagetitled Advancing Gender Equity in Academic Medicine also remains active, and is largely unchanged from previous iterations.
Additionally,the webpagefor the AAMC’s anti-racism resources no longer works. The website included a host of links to various articles, both internal and external, on the theory of “anti-racism,” including an article by Kimberlé Crenshaw, one of the leading scholars of critical race theory.
“Anti-racism,” according to its most prominent advocate, Ibram X. Kendi, is built on the idea that racial discrimination is essential and even praiseworthy, since it’s supposed to right past wrongs.
An older version of that webpage redirects to a webpage titled “Excellence in Academic Medicine.”
Figure 3. A screenshot of the AAMC’s “Anti-racism Resources” webpage.
Perhaps most interestingly, the webpage for the AAMC’s definition of “underrepresented in medicine” is no longer live.
“Underrepresented in medicine means those racial and ethnic populations that are underrepresented in the medical profession relative to their numbers in the general population,” the definition read.
Figure 4. A screenshot of the AAMC’s “Underrepresented in Medicine Definition” webpage.
However, the AAMC still maintains a definition of “underrepresented in medicine” on its FACTS webpage.
Even the AAMC’s news articles haven’t been safe; the AAMC removedan article titled “Do Black patients fare better with Black doctors?” that dealt with the notion that racial concordance, in which patients are treated by physicians of the same race, improves health outcomes.
That article featured prominently a discussion surrounding a now-debunked study that purported to show that black infants enjoy higher survival rates when treated by black doctors.
As Do No Harm covered in a recent report, the study in question spread like wildfire throughout the medical community, despite its findings being invalid.
Additionally, the AAMC has removed reports on its DEI competencies in medical education.
The AAMC’s report, Diversity, Equity, and Inclusion Competencies Across the Learning Continuum, now redirects to the Excellence in Academic Medicinelanding page.
Figure 5. A screenshot of the AAMC’s DEI competencies webpage.
The AAMC has also taken down all ten of the “Action Plan” elements of its “Strategic Plan” that included, among other things, pledges for the AAMC to take steps to increase diversity in medical education and medicine more broadly.
Action Plan item three, “Equip medical schools and teaching hospitals and health systems to become more inclusive, equitable organizations,” is no longer available on the AAMC website.
Figure 6. A screenshot of the AAMC’s Action Plan item three webpage.
Similarly, Action Plan item four, “Increase the diversity of medical school applicants and matriculants,” has been removed.
The item was active as of March 2025.
“By galvanizing the expertise of its member institutions and developing strategic partnerships, this action plan endeavors to make the pathway to the health professions more accessible, equitable, attainable, and desirable for underrepresented populations and historically marginalized communities,” the item read. “The AAMC is uniquely positioned to drive this initiative because of its robust repository of aspirant applicant and enrollment data, extensive analysis of trends in the physician workforce, relationships with experts in higher education, health care, and policy, and proven success with facilitating critical and crucial conversations.”
“Continue working with subject matter experts from our member institutions to identify and build out systems-based resources to implement holistic review with fidelity, to discuss impact of SCOTUS decisions, and to support and graduate a diverse cohort in an equitable manner,” one vow from the now-defunct page read.
Yet while these overt endorsements of DEI may be removed, many of the AAMC’s DEI initiatives remain.
For instance, the AAMC’s Action Collaborative for Black Men in Medicine, which is explicitly designedto “increase the representation of Black men in medicine,” remains active.
Additionally, the AAMC’s “Medical Minority Applicant Registry” is also still accessible on the organization’s website.
This tool is explicitly designed to get students from “historically underrepresented” into medical school; the eligibility criteria state that students must either be “economically disadvantaged” or members of underrepresented racial groups such as “African-American/Black, Hispanic/Latino, American Indian/Alaska Native or Native Hawaiian/Pacific Islander.”
“If you choose to participate in Med-MAR, your basic biographical information and your MCAT® scores will be distributed to the minority affairs and admission offices of AAMC-member schools and to select health-related agencies whose mission is to increase opportunities for students historically underrepresented in medicine,” the description of the tool reads.
While the AAMC removed the Action Plan item that created its Center for Health Justice, led by Dr. Philip Alberti, the center itself appears to still be operational.
Dr. Alberti madeseveral incendiary comments on a recent podcast, such as blaming problems with American healthcare on “isms” like “cisgenderism.” Additionally, the Center for Health Justice put out a language guide titled “Advancing Health Equity” intended to instruct healthcare professionals on the correct nomenclature to use to advance DEI ideals.
Additionally, the AAMC has left up its webpage an article titled “6 common myths about diversity in medical education.” The resource is a full-throated defense of DEI in medical education and uses misleading arguments to advance the DEI agenda. Do No Harm debunkedthe AAMC’s reasoning in a blog post last year.
Editor’s note: This article has been updated to include additional context surrounding the AAMC’s definition of “underrepresented in medicine.”
https://donoharmmedicine.org/wp-content/uploads/2025/04/shutterstock_663739642-scaled-e1745267226110.jpg10671860Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-06-17 13:08:132026-02-11 15:34:07The AAMC is Scrubbing Evidence of Its DEI Infatuation – But It’s Still There
The Sunshine State just took another major step toward eliminating DEI.
Florida lawmakers approved a budget Monday that takes major steps to prevent taxpayer dollars from subsidizing diversity, equity, and inclusion initiatives.
Legislation implementing the budget includes a provision ensuring state funds are spent in accordance with principles of individual freedom.
These include items such as the principle that no person should be discriminated against on the basis of their race, that no person is inherently racist or sexist (whether consciously or unconsciously), and that a person should not be instructed to feel guilt for actions committed by members of the same race.
These statements are antithetical to the DEI ideology, which posits that racial discrimination is often necessary to achieve equity, equalize outcomes, and remediate past wrongs.
Additionally, the budget includes language enablingGovernor Ron DeSantis to investigate local governments for spending state dollars on DEI programs.
Ensuring taxpayer dollars aren’t bankrolling discriminatory and divisive ideologies is important to ensure the integrity of publicly-funded medical education.
And it’s all the more important in Florida; as Do No Harm revealedthrough leaked audio recordings Dr. Haywood Brown, a former official and professor at the University of South Florida, delivered his advice on how to skirt the state’s anti-DEI laws at a Virginia Commonwealth University medical school grand rounds session.
It’s simple: taxpayers should not be forced to subsidize initiatives and programs that foment division and encourage racial discrimination.
https://donoharmmedicine.org/wp-content/uploads/2023/05/shutterstock_510558802-scaled.jpg17002560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-06-17 12:01:502026-02-11 15:34:06Florida Budget Prevents Tax Dollars From Funding DEI
This week, Do No Harm filed an amicus briefin support of Jennifer Vitsaxaki’s lawsuit against her daughter’s school district for “secretly transitioning” her daughter without Vitsaxaki’s consent.
The case, Vitsaxaki v. Skaneateles Central School District, concerns Vitsaxaki’s fundamental parental rights under the Constitution.
Employees at Vitsaxaki’s daughter’s school, acting under Skaneateles Central School District official policy, had been secretly referring to her 12-year-old daughter as a boy, such as through the use of a masculine name.
This so-called “social transition” was done without Vitsaxaki’s knowledge or consent; employees allegedly concealed this behavior from Vitsaxaki and continued doing it without her consent.
Vitsaxaki sued the school district, arguing that the school district’s policy violated her parental rights under the Fourteenth Amendment.
The district court granted the school district’s motion to dismiss the case, and Vitsaxaki appealed the decision to the U.S. Court of Appeals for the Second Circuit.
Do No Harm’s amicus brief urges the Second Circuit to reverse the district court’s decision, arguing that because Vitsaxaki alleged a violation of her fundamental constitutional rights that are “deeply rooted in our history and tradition,” the “strict scrutiny” standard should apply. This means that the school district’s policy must further a compelling state interest in order to be permissible.
Moreover, social transition invariably increases the risk of medical harm.
The natural conclusion of affirming a child’s self-professed “gender” is to place children onto the transgender medicalization pathway, in which they undergo invasive medical interventions to alter their body in accordance with their self-identified “gender.”
Protecting children from their parents thoughtlessly and automatically affirming their gender dysphoria is an important first step to prevent further harmful medicalization.
https://donoharmmedicine.org/wp-content/uploads/2024/06/shutterstock_2148891659-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-06-13 18:43:572026-02-11 15:34:06Do No Harm Submits Amicus Brief in ‘Secret Transition’ Lawsuit Against School District
Welcome news for parents and children in Southern California: Children’s Hospital Los Angeles (CHLA), one of the chief providersof child sex change services, is shuttering its program providing so-called “gender-affirming care” for minors, according to The Los Angeles Times.
The decision is due to a number of actions taken by the Trump administration to crack down on federal funding of dangerous and experimental gender procedures.
“These threats are no longer theoretical,” hospital executives said in an email to patients. “Taken together, the Attorney General memo, HHS review, and the recent solicitation of tips from the FBI to report hospitals and providers of GAC strongly signal this Administration’s intent to take swift and decisive action, both criminal and civil, against any entity it views as being in violation of the executive order.”
The email refers to the recent Department of Health and Human Services (HHS)reportwhich reviewed the ethics and evidence behind “gender-affirming care” and found that the “affirmation” approach to pediatric gender medicine “lacked sufficient scientific and ethical justification.”
CHLA’s pediatric gender clinic, The Center for Transyouth Health and Development, is helmedby Dr. Johanna Olson-Kennedy.
Last year, The New York Times reported that Olson-Kennedy had initially refused to publish the results of a multi-million dollar, federally-funded study that found that “puberty blockers did not lead to mental health improvements” in children; Olson-Kennedy’s decision was due to fears that the results could undermine the argument for “gender-affirming care.”
The results of thestudy were finally released earlier this month, finding that children’s depression symptoms and emotional health “did not change significantly over 24 months” of being on puberty blockers.
Olson-Kennedy was also sued for medical negligence by a woman who alleged that Olson-Kennedy’s clinic put her on puberty blockers when she was 12 and performed a double mastectomy on her at 14.
CHLA is one of the most prolific and prominent providers of so-called “gender-affirming care” in the country.
According to insurance claims datacompiled in Do Harm’s Stop the Harm Database, between 2019 and 2023 CHLA performed surgical procedures on over 160 patients under the age of 18.
And according to The Los Angeles Times, CHLA’s pediatric gender clinic provides services to nearly 3,000 patient families.
https://donoharmmedicine.org/wp-content/uploads/2025/06/shutterstock_2076463606-scaled.jpg16902560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-06-13 15:30:122026-02-11 15:34:06Children’s Hospital Los Angeles Will Stop Performing Child Sex Change Interventions