The nation’s largest not-for-profit healthcare organization is pushing “gender” radicalism on teens. This represents an unacceptable substitution of progressive ideology for medical science.
Among Kaiser Permanente’s patient offerings in its Northern California region are “Well Visits for Teens 12 to 18,” recommended every one to two years and focused on “keeping your teen healthy.”
According to the organization’s website, these visits largely involve standard care. Doctors “[c]heck your teen’s growth and development,” “[d]o a physical exam,” “[p]erform standard screening tests,” and “[m]ake sure vaccinations are up to date.”
All well and good so far — these are necessary, beneficial procedures. The trouble comes with the “brief questionnaire” that teens complete before their visit, a copy of which was recently obtained by Do No Harm.
The questionnaire introduces grossly inappropriate “gender” nudges into the doctor-and-minor-patient relationship.
Scattered among its mostly anodyne queries (e.g., “Do you usually eat at least 5 servings of fruits and vegetables each day?”) are items that present transgenderism as a normal possibility that every teen should confront.
Specifically, the questionnaire lists, on page two, in items 12 and 13, a series of “gender” options that are entirely at one with the ideology of the radical Left.
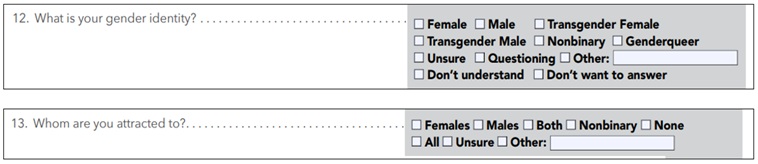
Imagine the 12-year-old faced with these questions and prospective answers.
Perhaps he or she has read about “gender identity” online and absorbed the generalities of the debate, but here is a physician coming in full authority to settle the matter.
“Genderqueer,” for example, is no longer an abstract category but something that an authoritative, highly trained adult thinks our young patient might reasonably be.
One needn’t spend a lifetime studying human nature to grasp that children are suggestible and that even to ask these questions is to put one’s finger on the scale of a fraught culture-war debate that has far less to do with medicine than with politics.
Moreover, the page of the questionnaire dealing with “gender” issues is explicitly presented as our little secret.
Whereas questions about diet, exercise, grades, and seat-belt usage are marked “Non-Confidential,” the aforementioned “gender” queries have a “Confidential” designation — as do questions about suicidal ideation, sexual activity, and intimate-partner violence.
This aligns with a notice posted back on the “Well Visits” page: “To respect your teen’s independence and privacy, we’ll see your teen alone for part or all of the visit.”
To an extent, this makes sense. If a 17-year-old is sexually active, he or she is taking on health risks and responsibilities that his or her physician conceivably ought to know about.
A real discussion is needed, and, at least in some families, the presence of Mom or Dad in the examination room might inhibit it.
This is a far cry, however, from the sneaky introduction of “gender” ideology to a 12-year-old. Not for nothing have states begun enacting parental-notification laws addressing the social “transitioning” of minors and opening up medical records to legal guardians. Parents have every right to know whether, when, and how their kids are being made to question the “alignment” of their biological sex and “gender identity.”
Finally, maneuvering of this kind on the part of physicians is destructive for broader reasons. It is a good thing if Americans trust their doctors. But how will we if healthcare providers come to be seen as ideological agents who can’t be trusted in a room with our kids?
In short, what Kaiser is doing isn’t just bad news for minor patients and their families. It is a threat to the basic trust that makes clinical care possible.
Do No Harm Calls on 10 Prominent Medical Organizations to End Support for Genital Surgery on Minors for the Purpose of So-Called Gender-Affirming Care
COMMENTARY Gender Ideology American Academy of Family Physicians, American College of Physicians, American Medical Association Medical association Press Release Do No Harm StaffSALT LAKE CITY, UTAH: July 29, 2026 – Today, Medical watchdog Do No Harm sent a letter to 10 major medical societies, urging them to reject genital surgeries on minors for the purpose of “gender-affirming care.”
Signed by Dr. Stanley Goldfarb, board chairman of Do No Harm, and Dr. Kurt Miceli, chief medical officer at Do No Harm, the letter calls on the organizations to recognize the commonsense idea that adolescents are not equipped to make informed decisions about such invasive and high-risk procedures and requests that the organizations remove these procedures as an option in any clinical-care plans or treatment protocols related to “gender-affirming care.” Children should not be subjected to unwarranted, irreversible procedures that remove healthy body parts, such as castration or hysterectomy.
The letter warns: “If your society continues to support the entire program of so-called gender-affirming care, it implicitly maintains that the cosmetic outcomes produced by hormones and mastectomies, for instance, confer some form of medical benefit. Yet this position is not supported by nearly two dozen systematic reviews that have been published in this field. Moreover, genital surgery does nothing to alter a person’s outward public appearance and has been notorious for producing multiple complications, including fistulas and urinary complications.”
Do No Harm has done extensive work to put an end to mutilative surgeries on minors diagnosed with gender dysphoria, as seen in its in-depth Stop The Harm database, which exposes the medical entities that perform these invasive procedures.
“Professional medical societies that endorse so-called gender-affirming care in minors bear tremendous responsibility for the harm done to American children in the name of gender ideology,” said Dr. Kurt Miceli, chief medical officer at Do No Harm. “These societies shape professional standards through their policy directives, clinical guidelines, and public statements. In many cases they are viewed as the experts to whom providers, lawmakers, and the public defer judgment on the safety and efficacy of treatments. We therefore call on professional medical societies to begin to right wrongs and explicitly oppose the performance of transgender genital surgeries on minors. No high-quality evidence demonstrates that these surgeries have beneficial outcomes in children. Medical societies must be clear and state their firm opposition to these unscientific and harmful procedures.”
Do No Harm’s letter calls on the following organizations to renounce all genital surgeries performed on minors for the purpose of “gender-affirming care”:
Read the full letter here.
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. It has over 50,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 26 countries.
Kaiser Permanente Is Pushing Transgenderism on 12-Year-Olds
COMMENTARY California Gender Ideology Health system Commentary Do No Harm StaffThe nation’s largest not-for-profit healthcare organization is pushing “gender” radicalism on teens. This represents an unacceptable substitution of progressive ideology for medical science.
Among Kaiser Permanente’s patient offerings in its Northern California region are “Well Visits for Teens 12 to 18,” recommended every one to two years and focused on “keeping your teen healthy.”
According to the organization’s website, these visits largely involve standard care. Doctors “[c]heck your teen’s growth and development,” “[d]o a physical exam,” “[p]erform standard screening tests,” and “[m]ake sure vaccinations are up to date.”
All well and good so far — these are necessary, beneficial procedures. The trouble comes with the “brief questionnaire” that teens complete before their visit, a copy of which was recently obtained by Do No Harm.
The questionnaire introduces grossly inappropriate “gender” nudges into the doctor-and-minor-patient relationship.
Scattered among its mostly anodyne queries (e.g., “Do you usually eat at least 5 servings of fruits and vegetables each day?”) are items that present transgenderism as a normal possibility that every teen should confront.
Specifically, the questionnaire lists, on page two, in items 12 and 13, a series of “gender” options that are entirely at one with the ideology of the radical Left.
Imagine the 12-year-old faced with these questions and prospective answers.
Perhaps he or she has read about “gender identity” online and absorbed the generalities of the debate, but here is a physician coming in full authority to settle the matter.
“Genderqueer,” for example, is no longer an abstract category but something that an authoritative, highly trained adult thinks our young patient might reasonably be.
One needn’t spend a lifetime studying human nature to grasp that children are suggestible and that even to ask these questions is to put one’s finger on the scale of a fraught culture-war debate that has far less to do with medicine than with politics.
Moreover, the page of the questionnaire dealing with “gender” issues is explicitly presented as our little secret.
Whereas questions about diet, exercise, grades, and seat-belt usage are marked “Non-Confidential,” the aforementioned “gender” queries have a “Confidential” designation — as do questions about suicidal ideation, sexual activity, and intimate-partner violence.
This aligns with a notice posted back on the “Well Visits” page: “To respect your teen’s independence and privacy, we’ll see your teen alone for part or all of the visit.”
To an extent, this makes sense. If a 17-year-old is sexually active, he or she is taking on health risks and responsibilities that his or her physician conceivably ought to know about.
A real discussion is needed, and, at least in some families, the presence of Mom or Dad in the examination room might inhibit it.
This is a far cry, however, from the sneaky introduction of “gender” ideology to a 12-year-old. Not for nothing have states begun enacting parental-notification laws addressing the social “transitioning” of minors and opening up medical records to legal guardians. Parents have every right to know whether, when, and how their kids are being made to question the “alignment” of their biological sex and “gender identity.”
Finally, maneuvering of this kind on the part of physicians is destructive for broader reasons. It is a good thing if Americans trust their doctors. But how will we if healthcare providers come to be seen as ideological agents who can’t be trusted in a room with our kids?
In short, what Kaiser is doing isn’t just bad news for minor patients and their families. It is a threat to the basic trust that makes clinical care possible.
Do No Harm Files Complaints Against Two Health Systems for Discriminatory Medical-School Programs
COMMENTARY DEI Health system Press Release Do No Harm StaffSALT LAKE CITY, UTAH: July 28, 2026 – Today, Do No Harm filed complaints with the U.S. Department of Health and Human Services Office for Civil Rights (HHS-OCR) against Atlantic Health System and Nemours Children’s Health for operating racially discriminatory pediatric training programs for fourth-year medical students. The complaints call on HHS-OCR to investigate the programs’ preferences for “underrepresented” racial groups and find violations of federal anti-discrimination laws.
“It’s disappointing and concerning that prominent health systems continue to sort and value individuals based on their race when determining who can be awarded valuable learning opportunities,” said Dr. Kurt Miceli, chief medical officer at Do No Harm. “These programs are especially important for fourth-year medical students, offering meaningful clinical training experiences, while also giving students the chance to showcase their skills at potential future residency sites. One’s race has no bearing on whether he or she is able to provide high-quality care. Merit, academic excellence, and a commitment to serving patients must be the determinants when Atlantic Health and Nemours select the most qualified students for these programs, not identity politics.”
Atlantic Health System, a nonprofit hospital that receives substantial federal funding, claims that diversity is “at the core of what makes [it] great.” The system’s “Minority Visiting Clerkship Program” offers training in pediatric medicine and is an “exemplary” opportunity for fourth-year medical students to learn from medical staff. Students selected to participate are awarded inpatient residency rotations, an interview for full-time residency after medical school, mentorship, and valuable networking opportunities with hospital staff. To prioritize diversity and inclusivity, the program bases its selection process on race, restricting applicants to members of so-called underrepresented in medicine groups (URIM). As defined by the Association of American Medical Colleges (AAMC), URIM groups include American Indians, Alaska Natives, African Americans, Hispanics, Native Hawaiians, and Pacific Islanders.
Nemours Children’s Health is a nonprofit healthcare system that serves nearly half a million children across more than 70 locations in six states; trains nearly 2,500 medical students, residents, and fellows annually; and is supported by sizeable federal funding. Nemours aims to ensure “that health equity and inclusion goals are at the top of the organization’s short- and long-term planning priorities.” In an effort to “attack and manage the causes of racial health disparities,” Nemours operates the “Visiting Student Scholar Program,” which offers fourth-year medical students clinical and educational opportunities, professional mentorship, and a competitive stipend. Nemours limits applicants to medical students who are “underrepresented in medicine,” ensuring the eligibility of only a select group of individuals belonging to those “racial, ethnic, religious, socioeconomic, [and] ability” classes that Nemours prefers.
Both Atlantic Health System and Nemours discriminate against white applicants and members of other races they disfavor, blocking these individuals from an equal opportunity to access valuable career-training opportunities on the basis of race. The United States Supreme Court has been clear that efforts to purportedly ensure racial diversity or balance disparities provide no justification for race-based programs under Title VI of the Civil Rights Act of 1964. Such acts of discrimination are in direct violation of both Title VI and Section 1557 of the Affordable Care Act.
Click here to read the complaint against Atlantic Health System.
Click here to read the complaint against Nemours Children’s Health.
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. It has over 50,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 26 countries.
Accreditation Changes Are Coming
COMMENTARY DEI Liaison Committee on Medical Education accrediting organization, Federal government Commentary Executive Do No Harm StaffTwo months ago, negotiators on the Department of Education’s Accreditation, Innovation and Modernization (AIM) committee reached consensus on a much-needed overhaul of the nation’s higher-ed accreditation system. Reformers have reason to hope that long-awaited changes are on the policy horizon.
A Department of Education press release reveals the breadth of the proposed regulatory alterations. In addition to “ensuring that students can transfer credits that they have previously earned at other colleges,” AIM has agreed to
These are laudable goals, long pursued by opponents of the “Diversity, Equity, and Inclusion” (DEI) takeover of undergraduate and professional programs, including medical schools. As Education Under Secretary Nicholas Kent remarked about AIM’s work,
Do No Harm concurs. We note, too, that executive-branch pushback against DEI is already contributing to an environment in which accreditors abandon long-held “woke” positions.
For example, earlier this year, the Liaison Committee on Medical Education (LCME), the sole accrediting body for allopathic medical schools, quietly updated its 2027–2028 standards, removing the requirement that medical schools inject DEI-oriented content into their curricula.
That move was welcome, but so would be a regulatory landscape in which the LCME can’t force medical schools to indoctrinate students into a discriminatory ideology — not just one in which it chooses not to.
And while introducing a new programmatic accreditor to compete with the LCME would obviously be a major and complicated undertaking, it is reasonable for the federal government to pry open that door.
In a call with Do No Harm members and staff earlier this week, Under Secretary Kent suggested that, under the proposed rules, existing accreditors might move into the professional-program space, resulting in competition between accrediting bodies.
This, too, is good news. Rescuing medical schools from ideologically driven legacy groups may one day be the only reasonable choice left to reformers.
In the coming months, the Department of Education will receive and review public feedback on AIM’s work. If the department issues a final accreditation rule by Nov. 1, the changes will go into effect on July 1 of next year.
Do No Harm will certainly be weighing in. And we will be watching the process with eager anticipation.
‘Hardship’ Mustn’t Be Used as a Proxy for Race in Admissions
COMMENTARY California DEI University of California San Diego School of Medicine Medical School Commentary Do No Harm StaffEarlier this week, the UC San Diego School of Medicine made news for its use of what Assistant Attorney General Harmeet Dhillon is calling a “shadow application process” that “unlawfully judge[s] applicants for admission based on their race.”
Yet a wider look reveals that the centralized application service used by most U.S. medical schools may be committing a similar DEI-inflected error.
As reported in the New York Post and elsewhere, the U.S. Department of Justice Civil Rights Division’s July 20 letter to UC San Diego alleges that the medical school “intentionally discriminated against applicants by granting and denying admission based on their race.”
Specifically, the letter suggests that the School of Medicine used “applicant-submitted information related to overcoming a ‘hardship’” as a proxy for race and ethnicity. “Hardship categorization was used as a way to skirt [Students for Fair Admissions v. Harvard] by putting [underrepresented minorities in medicine] into their own subgroups and thus ensuring that more URMs received interviews.”
Disappointingly, the widely used American Medical College Application Service (AMCAS) employs similar “hardship” language in its 2027 application workbook.
There, in a section titled “Other Impactful Experiences,” applicants “provid[e] admissions officers with a snapshot of [their] lived experiences” and “provide additional context about the challenges they may have experienced during their lives.”
The section is explicitly intended to identify candidates who have “faced challenges in various areas such as family background … community setting … or other life experiences.”
Lest anyone miss the point, the instructions urge candidates to “consider whether this question applies to [them]” and reminds them that “[m]edical schools do not expect all applicants” to answer it.
Indeed, the section is intended only “for applicants who have overcome major challenges or obstacles.” Those who proceed have 1,325 characters — perhaps 200 words — to “[d]escribe the challenge(s) or hardship(s) [they] consider most impactful” in their lives.
AMCAS’s “hardship” question lets American medical schools clandestinely reintroduce race as a factor in admissions. And many medical schools are eager to take advantage. As Do No Harm’s Ian Kingsbury wrote last year, Freedom of Information Act requests to the nation’s 93 public medical schools produced the conclusion that “schools are at least skirting the Supreme Court’s [SFFA] decision, if not violating it outright.”
Now the U.S. Department of Education’s Office for Civil Rights is investigating five more medical schools over alleged violations of federal civil-rights law.
In a much-noted clause in the SFFA v. Harvard majority opinion, Chief Justice John Roberts declared that, while the affirmative-action regime long governing college admissions was no longer to be permitted, “nothing in this opinion should be construed as prohibiting universities from considering an applicant’s discussion of how race affected his or her life, be it through discrimination, inspiration, or otherwise.”
But Roberts went on: “[U]niversities may not simply establish through application essays or other means the regime we hold unlawful today.”
If medical schools are not honoring that fine distinction, the time has come to hold them accountable. No matter how it is disguised, racial discrimination in admissions cannot be tolerated.
Do No Harm Files Complaint Against Two Oklahoma Schools for Discriminatory Nursing Scholarship Program
COMMENTARY Oklahoma DEI Public university Press Release Do No Harm StaffSALT LAKE CITY, UT; July X, 2026 – Today, Do No Harm filed a complaint with the U.S. Department of Education Office for Civil Rights (ED-OCR) alleging that Northeastern State University (NSU) and Northeastern Oklahoma A&M College (NEO) unlawfully discriminate on the basis of race in a nursing scholarship program offered solely to American Indian students.
Both schools receive federal funding and are subject to federal civil rights laws. Do No Harm’s complaint alleges that the schools’ program — the Northeast Oklahoma Recruitment and Advancement of American Indians into Nursing (NEORAAIN) program — violates Title VI of the Civil Rights Act of 1964 through the exclusion of all students who are not of American Indian descent. The program covers tuition, books, fees, and living expenses for recipients of the award in addition to providing mentorship and access to professional events.
“NSU and NEO are excluding qualified individuals from rich learning opportunities based solely on race, regardless of their academic ability, skills, experiences, and perspectives and even if they commit to serving in Indian health facilities,” said Dr. Kurt Miceli, Chief Medical Officer at Do No Harm. “Favoring one race over all others is not only unlawful and unjust but also discredits the value of hard work and meritocratic achievement that is critical to our healthcare-education system. Do No Harm urges both universities to reverse their discriminatory ways and recenter their nursing scholarship program around excellence and academic rigor.”
The NEORAAIN program advances discrimination by offering scholarship opportunities to some students rather than others on the basis of race. The program aims to:
Do No Harm’s complaint argues that the NEORAAIN program’s preferences have no legally justified basis and requests that the ED-OCR investigate NSU and NEO and find that their race discrimination violates Title VI.
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. It has over 50,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 26 countries.
The Chloe Cole Act Rolls On
COMMENTARY Gender Ideology Federal government Commentary Legislative Do No Harm StaffThe Chloe Cole Act of 2026 has cleared an important legislative hurdle and is one step closer to becoming law. Americans eager to protect children from transgender ideology should celebrate.
Introduced by Rep. Bob Onder (R-Wis.) and co-sponsored by 86 other House Republicans, H.R. 7651 establishes a private right of action enabling children, parents, or guardians to sue providers of transgender surgeries or other interventions that were performed on minors.
The bill cleared the House Judiciary Committee on a party-line vote last Wednesday and now heads to the House Rules Committee, the last step before consideration by the full House.
In a statement released by the Independent Women’s Forum, Rep. Onder expressed his dismay “that politics and ideology have been allowed to override sound medical judgment, leaving vulnerable children to undergo irreversible procedures without a comprehensive psychological evaluation, treatment of underlying mental health conditions, or truly informed parental consent.”
The Chloe Cole Act, he continued, “would allow families to hold clinics and hospitals accountable and ensure victims have adequate time to seek justice.”
Do No Harm agrees. In his own statement, Chief Medical Officer Kurt Miceli, MD, noted that “[p]assing The Chloe Cole Act will not only establish a strong deterrent against sex‑rejecting procedures in minors by exposing harmful actors to real legal accountability but also mark a meaningful step toward justice for those harmed by the child sex‑change industry.”
H.R. 7651 is an attempt to implement at the federal level what a number states have already done. Among the states that have passed into law a similar private right of action are Arkansas, Iowa, Indiana, Kentucky, Louisiana, Missouri, Mississippi, North Carolina, Nebraska, Oklahoma, and Tennessee. Montana’s law creating one has been blocked by its state Supreme Court.
Though these piecemeal efforts are welcome, they create a two-tiered system in which red-state children are protected from ideological manipulation concerning “gender,” while blue-state children are not.
The Chloe Cole Act is an attempt to remedy this situation, because all children deserve these protections regardless of where they live, and minors who have been harmed need justice.
What is the Act’s likely legislative future? Regrettably, the House Judiciary Committee advanced the bill on a party-line vote, with no Democrats voting in support of the measure. The bill has no Democratic cosponsors. No Democratic senators have spoken in favor of the Act, and one struggles to imagine that 60 votes will be found to achieve Senate cloture, even if the House passes the bill successfully.
Nevertheless, the effort is worthy and essential. Opponents of sex-rejecting procedures for minors need allies wherever we can find them. The American litigation system could be an effective one, and this Act would open it up to all children and their families.
Gender Madness at the American Society of Pediatric Hematology/Oncology
COMMENTARY Gender Ideology Medical association Commentary Do No Harm StaffThe American Society of Pediatric Hematology/Oncology (ASPHO) describes its annual gathering as the “leading education conference” in its field. That makes the society’s commitment to leftist race and gender orthodoxies all the more troubling.
Scheduled for May 11–14, 2027, ASPHO’s next conference will feature “educational/scientific workshops” comprising “interactive, problem-solving discussions, debates, or cases.”
Conference organizers urge workshop proposers to “seek speakers from a diverse group of faculty,” considering not only the “institution size” and “career level” of prospective panelists but their “gender” and “race/ethnicity,” as well.
Although this policy represents a lamentable emphasis on identity categories rather than scientific merit, it is par for the course given the woke-era politicization of medicine. What is less predictable — and at least as troubling — is the “previously accepted, well-received workshop proposal” offered as a sample to attendees.
That proposal, titled “Hematology Consults in Transgender Medicine,” notes that many of the “10% of high school students [who] identify as gender non-congruent … are transgender,” a state of affairs that leads “to an increased use of medications with potentially serious hematologic adverse effects (thrombosis, erythrocytosis, etc.).”
According to the proposal, hematologists “are being asked to provide consultation to the transgender community regarding critical management questions” and should know “how to mitigate the risks of such treatments.”
This is precisely the opposite of how medical care should work. Yes, practitioners should be aware of the side-effects of the interventions they propose, but “risk mitigation” makes no sense given the very low certainty that pediatric transgender medicine offers meaningful psychological or quality-of-life benefits at all.
If, as a 2021 medical study showed, “data indicat[e] higher rates of venous thromboembolism (VTE) and ischemic stroke (IS) among [biologically male] participants receiving [hormone therapy],” then that is an argument against prescribing estrogen to high-school boys. It is not an argument for “mitigat[ing] the risks” of such “treatment.”
Similarly, if, as another 2021 medical study found, “[e]rythrocytosis occurs in trans men using testosterone,” then the role of physicians should be to prevent that outcome in children, not to manage it.
Sadly, ASPHO’s sample proposal is more concerned with “appropriate terminology” than with preventing harm to gender-dysphoric children and adolescents in the first place. Of the proposal’s three “learning outcomes,” two concern the language used by hematologists (e.g., “the new gender-neutral hemophilia nomenclature”).
These confused values are as unsurprising as they are disappointing.
According to the organization’s “Diversity, Equity, & Inclusion at ASPHO” page, DEI is “infused into the Society” through a diversity advisory group and regular diversity-themed webinars and “eNews” statements.
The same page offers a link to the debunked “Implicit Association Test” beloved by activist progressives.
Even an entirely legitimate and beneficial medical pursuit is framed using “antiracist” terminology: “We Must Support Black Lives to Improve Sickle Cell Disease Care.”
In short, ASPHO’s medical expertise appears increasingly to be giving way to leftist ideology. That is bad news for pediatric hematology/oncology patients, as well as for the broader medical and scientific establishments.
Like all Americans, physicians have every right to their individual political beliefs. When entire medical societies allow politics to corrupt their work, however, we are all in trouble.
At the University of Chicago’s Pritzker School of Medicine, Mixed Signals on ‘Inclusion’
COMMENTARY Illinois DEI Medical School Commentary Do No Harm StaffWhat happens when a DEI committee co-opts the language of the right while otherwise maintaining a standard-issue leftist perspective? The University of Chicago’s Pritzker School of Medicine seems to be running that experiment.
Pritzker’s Identity and Inclusion (i2i) Committee is not to be confused with its Health Equity, Diversity, and Inclusion office, a separate administrative unit straightforwardly dedicated to the principles of DEI.
Rather, i2i is a steering committee comprising faculty and staff members, student “affinity group” representatives, and members of the “student governance, wellness, and curriculum committee[s].” The body is “responsible for providing ongoing direction for programs and/or curricula at Pritzker that support an inclusive learning environment and promote respectful and effective communication with diverse patients and colleagues.”
One sees right away the tension baked into i2i’s mission. “Respectful and effective communication” is an obvious good in the realm of medical education. An “inclusive learning environment,” conversely, is too often a stalking horse for unscientific and discriminatory DEI initiatives.
Closer examination of i2i’s activities produces further confusion. The committee develops “civil discourse” resources, in which “diversity of thought … [is] valued.”
It arranges “civil discourse events,” a move that calls to mind much-lauded initiatives by education reformers to break the progressive stranglehold on campus speech.
Yet this encouraging language is surrounded on i2i’s website with ideas that wouldn’t be out of place in the farthest-left DEI bodies in America.
The committee “[e]nhanc[es] cultural competency training during Free Clinic Orientation.”
It provides “[t]raining in bias and identity issues that affect patients during the Clinical Skills course sequence.”
It “[i]dentif[ies] speakers to give foundational lectures on the nature of self and identity.”
It conducts an “annual student-led climate survey” and hosts an “all-school town hall to review the survey results.”
These are poor initiatives, proceeding directly from the same DEI mindset that produces racially discriminatory hiring and recruiting policies and identity politics in the classroom.
Trainings in “cultural competency,” for example, risk reducing patients to demographic labels, treating identity as a clinical shorthand instead of engaging with the complexity of patients’ individual histories, preferences, and beliefs.
Similarly, training in “bias” often presumes that clinician prejudice — implicit or otherwise — is the primary cause of any noted disparity, downplaying or even ignoring factors such as patient behavior, cultural practices, genetic variation, etc.
“Lectures on the nature of self and identity” belong in the philosophy classroom, not the medical school.
So-called climate surveys seem harmless enough until one recalls Texas A&M’s infamous (and disastrous) attempt to “fix” its own climate “problems.” To the extent that the disease existed in the first place, it was far less unpleasant than the cure.
Pritzker should go out of its way to avoid similar trouble. Indeed, its i2i committee’s pronouncements on civil discourse suggest that at least some reasonable notions have support on campus.
A word to the wise, however: DEI ideologies and civil discourse cannot coexist forever. An institutional commitment to the former soon makes the latter impossible.
Do No Harm Supports the Chloe Cole Act
COMMENTARY Gender Ideology Federal government Press Release Do No Harm StaffStatement by Dr. Kurt Miceli, Chief Medical Officer at Do No Harm, in support of the Chloe Cole Act:
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. It has over 50,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 26 countries.
Please view Dr. Miceli’s formal statement here and below.
Do No Harm Files OMB Comment on Federal Funding of Chemical and Surgical Mutilation of Children
COMMENTARY Gender Ideology Federal government Commentary Executive Do No Harm StaffTwo days ago, Do No Harm answered the Office of Management and Budget’s (OMB) request for comment on a proposed rule to ensure that federal funding does not support the chemical and surgical mutilation of children under 19 years of age.
Specifically, OMB proposes requiring federal agencies or pass-through entities to verify that government funds are not supporting “the so-called ‘transition’” of minors.
Do No Harm fully supports this effort.
To begin with, scientific evidence does not validate the procedures in question, which can include the use of puberty blockers, cross-sex hormones, and invasive surgeries that attempt to physically reject a child’s biological sex.
Furthermore, and consequently, funding these procedures contradicts the government’s commitment to support science-based medicine. Sex-rejecting procedures for minors are ideological, not scientific.
Finally, by directing agencies and recipients — unless expressly required by law — not to use federal awards to support “disparate-impact” studies, litigation, or related activities, the proposed rule reasonably seeks to prevent federal funding from creating race-conscious incentives in medicine. Do No Harm strongly supports this prohibition.
Please read the full comment here or below.
Do No Harm Report Exposes Rise in Woke and Weak Research by Medical Students
COMMENTARY DEI Medical Journal, Medical School Press Release Do No Harm StaffSalt Lake City, UT: July 14, 2026 – Today, Do No Harm released a report that exposes how low-quality medical student–authored research has increased over the last two decades, corresponding with medical schools’ elimination of letter grades. The report concludes that the increased volume of studies authored or co-authored by students is driven by their desire to pad their résumés in the absence of other academic distinctions. Moreover, the student research in question is disproportionately focused on politicized topics.
The report, titled “Why Johnny Can’t Stop Writing: The Boom in Low-Impact, Politicized Medical-Student Research,” conducts an advanced search through the medical-journal database PubMed to identify publications authored by medical students and, separately, those that use politicized terms such as “equity,” “justice,” “racism,” and “diversity.”
“Without the use of the letter-grade system, students are searching for other ways to stand out for fellowships and residency programs, which has inevitably led to an arms race in publications authored by medical students,” said Jay Greene, PhD, Director of Research at Do No Harm. “To compound the problem, quantity is incentivized over quality — leading to shoddy research and focus on politicized topics. Our report reveals the many factors responsible for the degradation of the research enterprise and offers proposed solutions to correct course. By returning to objective letter grading, schools would incentivize students to focus on mastering their skill set in the clinical space rather than fluffing their résumés with baseless research endeavors.”
Click here to read the full report.
The report also conducts a thorough analysis of two competing studies. The first, by Hausner et al., concludes that medical research grew in both volume and quality between 2003 and 2023. The second, by Elliott et al., finds that the rise in student-authored articles led to a notable decline in quality. Do No Harm’s analysis concludes that the Hausner study excluded 72 percent of medical-student publications in its analysis, distorting its findings, In addition, the primary metric used in the Hausner study, Relative Citation Ratio (RCR), is an unreliable indicator of article quality.
The report cites several examples of low-quality and politicized research, calls for medical students to redirect their time and energy toward excelling in coursework and acquiring the knowledge needed to be excellent physicians, and furthers Do No Harm’s larger mission to depoliticize medical research and recenter medical education on rigor and skill.
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. It has over 50,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 26 countries.
Do No Harm Files FDA Comment on ‘Sex’ Versus ‘Gender’
COMMENTARY Gender Ideology Federal government Commentary Executive Do No Harm StaffLast week, Do No Harm submitted to the U.S. Food and Drug Administration a comment in support of a proposed rule replacing “gender” with “sex” — or removing “gender” altogether — throughout Title 21 of the Code of Federal Regulations.
The proposed change follows the directive of Executive Order 14168, “Defending Women From Gender Ideology Extremism and Restoring Biological Truth to the Federal Government,” issued on January 20, 2025.
It also aligns with scientific evidence.
Per the executive order: “[E]very agency … shall use the term ‘sex’ and not ‘gender’ in all applicable Federal policies and documents.”
This is important because sex (not “gender”) is a primary variable that affects pharmacokinetics — i.e., the movement of drugs through the body. Clinical studies, prescription labeling, and adverse-event reporting can all be compromised when differences between the two sexes — men and women — are improperly indicated or not taken into account.
At stake here is women’s health. The safety and efficacy of medical treatments should not be sacrificed in furtherance of gender ideologies.
Please read the full comment here or below.
SUNY Medical Schools Have Embraced DEI. Blame SUNY.
COMMENTARY New York DEI State University of New York, SUNY Downstate Health Sciences University College of Medicine, SUNY Upstate Medical University Norton College of Medicine Medical School, Public university, University System Commentary Do No Harm StaffIncluded among the State University of New York’s (SUNY) constituent institutions are four medical schools. All four express a commitment to wokeness in the form of DEI.
At best, these gestures are vogue frivolities — concessions to an activist class that demands ideological tribute from public institutions.
At worst, they are actively harmful, leading to discrimination in favor of some people and against others in an attempt to address different outcomes among racial groups.
Yet attempts by reformers to address this behavior at SUNY’s medical schools will necessarily be an uphill battle. The reason? SUNY itself has been captured by ideological forces intent on the widespread introduction and defense of DEI.
The evidence is unignorable:
Nor are things better at many of SUNY’s individual campuses:
This is one of the ways in which activists perpetuate DEI ideology. By gaining a foothold both at the senior administrative level of SUNY and in the individual SUNY campuses, bad actors make it next to impossible for dissenting administrators and campuses to resist (assuming any such individuals or institutions exist).
In other words, a SUNY medical school that wished to dispense with unscientific DEI frippery would be swimming upstream. All the momentum is going in the other direction.
To be clear, this doesn’t mean that reformers’ task is hopeless. But it does mean that we have a long road ahead of us.
North Carolina’s New Medical School Is Already Woke
COMMENTARY North Carolina DEI Medical School Commentary Do No Harm StaffMethodist University’s new Cape Fear Valley Health School of Medicine has recruited its inaugural class of students and will begin instruction later this month. Unfortunately, the budding institution appears to have laid a foundation of DEI.
Located in Fayetteville in south-central North Carolina, Methodist’s new School of Medicine was created in part to address a physician shortage east of the state-bisecting Interstate 95. As such, one might expect (and indeed one finds) an emphasis on the healthcare needs of a particular set of people in the institution’s materials.
Methodist SOM’s job page, for example, cites its “clear mission to prepare graduates who are … community-engaged.”
The institution’s “Mission, Vision & Values” page specifically notes that, “[i]n non-metropolitan counties in North Carolina, growth in physicians-per-capita has been slow” and that “[t]he University’s … medical school will be perfectly positioned to address this deficiency.”
The new school intends to prepare graduates “who will contribute to … improving health outcomes … wherever they may practice.” Nevertheless, “southeastern North Carolina” receives a particular nod.
None of this is undesirable. Regional physician shortages are real, and a medical school created to address that gap has every right to hold to a community-focused mission.
The problem occurs when an appropriate regional focus gives way to inappropriate DEI ideology.
That is already happening at Methodist SOM. The previously cited job page, for instance, mentions not only “community-engaged” graduates but graduates who are “focused on equity.”
The page boasts of Methodist SOM’s “Diversity & Inclusion Initiatives,” noting its “targeted recruitment and retention efforts aimed at ensuring a diverse faculty and student body.”
Over on the “Mission, Vision & Values” page, site visitors learn that graduates should be “equity-focused physician leaders who will contribute to mitigating health disparities.”
Because the institution intends to “educate a diverse population,” it lists among its “Values” a desire for “Inclusive Belonging.”
One might reasonably ask what any of this has to do with medical science. Indeed, like most of the doctrines of the “Diversity, Equity, and Inclusion” movement, this thinking has at its core the assumption that “systemic” forces have created racist outcomes that only social engineering can address.
If that proposition is true, then DEI advocates should produce the evidence. That they are unable to do so reveals much about the ideological (rather than scientific) nature of their claims.
Nevertheless, Methodist’s new medical school appears to be constructing a DEI apparatus that may already be affecting hiring and admissions. Regarding the latter, consider the words of Hershey Bell, MD, the institution’s dean: “What stood out” as Methodist SOM measured applicants “was not just academic excellence, but alignment with our mission.”
It may well be the case that south-central and southeastern North Carolina need a medical school. But they don’t need a woke one.
A Victory for Science and Fairness in Women’s Sports
COMMENTARY Idaho, West Virginia Gender Ideology State government Commentary Judicial Do No Harm StaffOn June 30, the Supreme Court ruled in West Virginia v. B.P.J. and Little v. Hecox that neither Title IX nor the Equal Protection Clause prevent states from providing separate men’s and women’s sports teams on the basis of biological sex. Notably, since approximately 2020, 27 states have enacted legislation to maintain female sports for biological females. The judgment is a victory for common sense.
The consolidated cases were brought by male athletes who wished to compete on female sports teams on the basis of their transgender identification. At issue was whether state laws in West Virginia and Idaho that prevent such an outcome discriminate on the basis of sex in violation of federal civil-rights laws and the Constitution.
In a unanimous 9–0 ruling, the Court declared that the states’ laws enacting sex-separated athletics are indeed consistent with, and do not violate, Title IX. Delivering the opinion, Justice Brett Kavanaugh confirmed that “Title IX’s implementing regulations expressly permit schools to maintain separate teams for ‘members of each sex’” and that “the term ‘sex’ in Title IX cannot plausibly be interpreted to refer to anything other than biological sex.”
Moreover, on the constitutional question, the Court held 6–3 that sex-based classifications advancing safety and competitive fairness for biological women and girls are constitutionally sufficient interests such that states “d[o] not violate the Equal Protection Clause of the Fourteenth Amendment by maintaining female sports teams for biological females.”
This ruling comports with amicus briefs filed by Do No Harm. In our briefs in support of West Virginia and Idaho governor Bradley Little (R), we argued that sex and gender identity are fundamentally distinct and that altering the latter has no bearing on the former. (“Scientific facts do not change with the shifting winds of cultural ideology: An individual’s gender identity does not alter his or her sex.”)
We argued further that the lower court decisions in these cases “reflexively assumed that using puberty blockers and cross-sex hormones to treat gender dysphoria is beyond debate” and had effectively “eviscerat[ed] the entire idea of boys’ and girls’ sports teams.”
As Justice Thomas echoed in his concurring opinion: “Men and boys with gender dysphoria are not women or girls, even if they believe that they are. Sex is an immutable ‘biological’ characteristic; it is binary; and ‘man’ and ‘woman,’ ‘boy’ and ‘girl,’ are the terms that correspond to adults and children of each sex.”
Likewise, the Court specifically noted that even if the premise advanced by the transgender athletes were true — “that at least some biological males who identify as female and take puberty blockers or hormones do not retain physical advantages over biological females” — states would nevertheless be constitutionally justified in maintaining sex-separated sports teams on the basis of the important interests in advancing safety and competitive fairness for the female sex.
Importantly, the Court also noted that the issue of whether or to what extent differences are retained following the administration of puberty blockers or hormones is not a decided question and “is the subject of ongoing medical and scientific debate.” Courts should not take it for granted.
Do No Harm welcomes the Court’s straightforward reasoning and ruling. Yet we also look forward to the inevitable next question, helpfully previewed by a footnote in Justice Kavanaugh’s opinion:
The Court is, of course, correct. Having now confirmed that Title IX and the Constitution permit states to protect women’s sports from unfair and unsafe incursions by male athletes, courts will have to decide next whether states must do so.
America’s Medical Schools Tiptoe Away from DEI — For Now
IN THE NEWS DEI accrediting organization Op-Ed Stanley Goldfarb, MDRead more at the New York Post.
Another DEI Office Name Change at the University of Arizona College of Medicine-Tucson
COMMENTARY Arizona DEI University of Arizona College of Medicine Medical School Commentary Do No Harm StaffIn 2024, the Office of Diversity, Equity & Inclusion at the University of Arizona College of Medicine-Tucson (UACOM-T) was rebranded the Office of Access, Community & Belonging.
Since then, the administrative unit has been renamed the Office of Community Engagement & Partnerships.
We look forward to whatever it may be called next.
There is reason for our suspicion that UACOM-T is merely abandoning politically troublesome terminology. To begin with, and as Do No Harm has previously noted, the DEI office’s first name change was largely cosmetic.
While UACOM-T scrubbed several DEI resources from its website during the unit’s first evolution, the pages of the DEI office and the Access, Community & Belonging office contained numerous similarities.
Importantly, both offices were run by the same administrative official, Celina Valenzuela, MD.
Dr. Valenzuela remains the head of the new Office of Community Engagement & Partnerships and retains her title of “vice dean.” In a greeting posted on the office’s first two homepages, she professed that “Inclusive Excellence is fundamental to the advancement of science” and pledged support for “the active recruitment, training, and retention of a medical and research workforce that reflects the demographics of Arizona.”
These DEI-informed attitudes remain despite the office’s second name change. Indeed, they are all over the Office of Community Engagement & Partnership’s online home.
Among the first examples one notices is the new office’s “Land Acknowledgement,” unchanged since its days as the Office of Access, Community & Belonging.
The new office still offers a “Pathways to Success” program for high schoolers, composed, in part, of an event series in which “speakers highlight the importance of … representation and diversity in health care.”
The new office continues to brag that Pathways to Success “[p]rovides students from under-resourced backgrounds with a unique opportunity to explore careers in medicine,” “[e]ncourages [d]iversity in [m]edicine,” and “promote[s] long-term inclusivity.”
Tellingly, the Pathways to Success program is “particularly” for high-school juniors and seniors “[f]rom historically under-resourced communities,” a term of art that makes clear the office’s preference for applicants of certain races and ethnicities.
In its outreach to current medical students, the renamed Office of Community Engagement & Partnerships is similarly committed to the principles of DEI.
Among its sponsored organizations is a Student Council on Community Engagement, which “[p]romote[s] community-responsive care in the curriculum” and “[s]upport[s] [the] recruitment and retention of mission-aligned faculty/staff.”
“Community-responsive care,” while seemingly harmless, brings to mind the activist obsession with “social determinants of health” and the prioritization of “systemic” rather than behavioral threats to patient well-being. “Mission-aligned” thinking in hiring and admissions, meanwhile, is, in many cases, a workaround for decisionmaking based on race.
Also, why is a student-led group so intimately involved with curricular design and faculty recruitment practices? Wouldn’t those be the domain of the institution’s academic leadership and faculty — those entrusted with maintaining professional standards and stewarding the long‑term integrity of the program?
Perhaps most troublingly, through the new Office of Community Engagement & Partnerships, student groups may apply for funding for “student-led workshops or trainings on … advocacy [or] health equity.” While there is obviously nothing wrong with students forming campus groups, should a taxpayer-funded public medical school help pay for advocacy training?
This is the same DEI music sung to the same DEI tune. Only the name of the song has changed.
Yes, UACOM-T has once again renamed its diversity office. But the work goes on.