Does California ever get its fill of massive spending on woke health equity projects? Apparently not, according to the hundreds of millions of dollars the state is pouring into efforts to alter the way healthcare is delivered in medical practices.
The California Department of Health Care Services (DHCS), the self-proclaimed “backbone of California’s health care safety net,” is dedicating $700 million to a “practice transformation program” for primary care providers (PCP). Called the Equity and Practice Transformation (EPT) Payments Program, the goal is to promote health equity, align with the DHCS Comprehensive Quality Strategy and Equity Roadmap, and provide funding for PCPs whose practices serve Medi-Cal patients.
The state’s leading medical organization was at the forefront of agitating for this funding. As announced by the California Medical Association (CMA), the organization “heavily advocated for this funding during the budget process.”
So what do they hope to achieve?
“Sixty-eight percent of the Medi-Cal population is Black, Latino, or people of color,” the EPT guidebook states. Funding will focus on the “50 by 2025 Bold Goals,” which include reductions in racial/ethnic disparities in well-child visits and immunizations by 50%, as well as disparities in maternity care “for Black and Native American persons” by 50% at the state level.
Oddly, we saw no goal for closing maternity care disparities for Hispanic patients in the EPT guidebook.
Figure 1. DHCS “50 by 2025 Bold Goals” of the Equity and Practice Transformation Program.
That’s not the only glaring inconsistency in the EPT program. The guidebook refers to the “Scaling of Evidence-Based Models Pathway,” which is also fixated on the Bold Goals and lists “implementing group prenatal care (e.g., centering pregnancy or Black Centering)” as the first initiative. According to UCSF, “Black Centering” is part of a group-focused prenatal care model “in a racially and culturally safe space.”
Of even greater concern is that healthcare providers who participate in the program are reimbursed for services via a “pay for performance” incentive system. “Phase 2 requirements,” the guidelines state, “would include pay for performance incentives based off certain targeted quality measures.” Those metrics must be aligned with the 50 by 2025 Bold Goals.
The application process serves to identify PCPs who will buy into the conditions of the EPT program. Potential participants must complete the 50-question Population Health Management Capabilities Assessment Tool (PhmCAT), which assesses “eight common domains” influenced by the Population Health Management Initiative (PHMI). The PHMI is DHCS’s partnership with Kaiser Permanente and community health centers across California, and is designed for “emphasizing populations of focus where disparities exist.” Participating health centers will “collect and analyze REAL (race, ethnicity, and language) data and social needs data.” This is reflected in the PhmCAT survey.
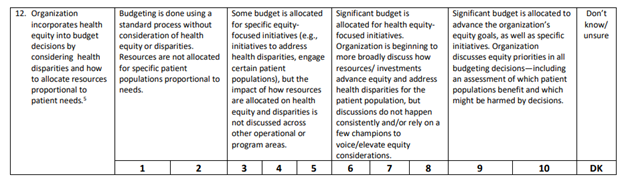
Among the questions related to operational workflows and resources, the survey asks about the practice’s dedication to providing “staffing, funding, and structures” to support DEI-related goals. Examples are “equity leads” and “internal equity workgroups.”
Figure 2. From the PhmCAT, Population Health Management Initiative (June 2023) – DEI goals.Figure 3. From the PhmCAT, Population Health Management Initiative (June 2023) – Budgeting for DEI initiatives.
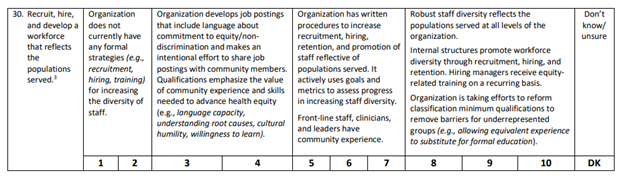
Recruiting and hiring practices are another theme of the survey, with the highest points earned for organizations that hire and promote staff based on DEI, as well as those that offer regular DEI-based training.
Figure 4. From the PhmCAT, Population Health Management Initiative (June 2023) – Recruiting and hiring practices.
The last group of questions on the PhmCAT focuses on “social health,” and the questions are based on information from a report by the National Academies. The report describes “social care integration” by healthcare systems “to improve the nation’s health and reduce health inequities.” In other words, doctors and other healthcare providers are told that addressing their patients’ “social determinants of health” is their duty in the name of health equity, despite having no agency to deal with these issues.
Figure 5. From the PhmCAT, Population Health Management Initiative (June 2023) – Addressing social needs.
Improving access to medical services is an important focus for all areas of healthcare. But are California’s Medi-Cal providers being incentivized to provide higher quality medical care to specified minority populations than other groups of patients? Are physicians and medical practices being told that they must act as social service providers for certain patients in order to receive optimal reimbursement? With the structure of the EPT program, DHCS is assuming that the cause of health disparities is largely due to the character of the healthcare system. Yet there is no evidence that any of the efforts the program promotes will actually improve health outcomes. There is a distinct difference in deploying initiative that improve access to care versus those that simply target increasing diversity and equity, which aims to change the nature of the patient/physician relationship.
Do No Harm is monitoring this situation. Please contact us if you’re a Medi-Cal provider with concerns about this program.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_429415330-scaled.jpg17002560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-09-14 12:12:312026-05-11 14:32:42California Medical Association Advocates for $700 Million Project for “Equity and Practice Transformation”