Would you want your psychiatrist viewing your treatment through the lens of historical racial inequities? Should your psychiatrist have spent their time learning how to incorporate “equity-focused language” into their practice?
The answers to these questions may seem obvious, but not to the University of Washington (UW).
The UW School of Medicine’s Department of Psychiatry and Behavioral Sciences has a “toolkit” for how to promote “equity, diversity, and inclusion” (EDI) within medical education.
The toolkit is specifically for the UW Psychiatry Residency Program, which has a “dedicated EDI module” within its didactic curriculum to promote DEI topics in medicine. According to the department’s DEI page, the module includes topics such as “structural competency, social determinants of mental health, bias in the clinical encounter, the Cultural Formulation Interview, an LGBTQ series, religion & psychiatry, ableism, the history of racism and sexism in psychiatry, cultural psychiatry, and global mental health.”
Additionally, the residency program also elects an “EDI Lead” in charge of the EDI/DEI initiatives within the program, including organizing “Antiracism Committee meetings,” organizing the “URM Support Group,” and assisting with recruiting efforts for “underrepresented applicants,” and improving the EDI didactic curriculum.
The URM Support Group appears to be a racial affinity group of some kind that the department describes as a “safe space for residents who are under-represented in medicine” that is “led by underrepresented alums of the program.”
It’s unclear what the membership criteria is for this group, and it does not appear similar resources exist for groups not deemed to be “underrepresented.” And the reference to recruiting efforts for “underrepresented applicants” smells like preferential treatment for individuals based on race.
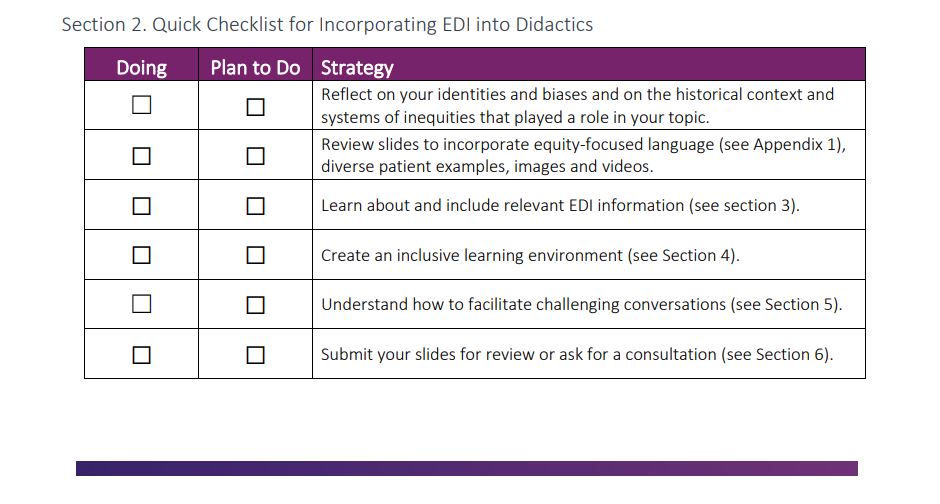
But that’s not all; the toolkit encourages residents to prioritize DEI concepts in medical education. For instance, the toolkit features a checklist that includes a reminder to “reflect on your identities and biases and on the historical context and systems of inequities that played a role in your topic.”
Figure 1. Screenshot of UW’s Checklist for Incorporating EDI into Didactics.
The toolkit further urges residents to “address equity by discussing how these systems of oppression came to be, continue to exist, and the ways we can help our patients overcome them.”
Residents can further advance DEI by “celebrat[ing] achievements made by diverse people and groups in psychiatry and mental health.”
The toolkit also includes a section on “gender equity,” in which it encourages the use of “inclusive terminology such as “people with the capacity for pregnancy” rather than “women” since, quote, “not all people who can become pregnant are women.”
In summation, the UW School of Medicine wants to reshape psychiatric education around a radical and divisive agenda that encourages discriminatory policies and beliefs.
These are not the best practices to treat patients’ mental health; rather, they are the hallmarks of ideologues using psychiatry to advance their worldview.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1845309475-scaled.jpg14402560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-02-19 18:04:222026-05-11 13:29:18University of Washington Injects DEI into Psychiatry