This past September, the University of Washington School of Medicine (UW Medicine) hosted its annual “Re-Imagining Behavioral Health: Race, Equity and Social Justice Conference,” offering attendees the opportunity to earn continuing education credits. The explicit purpose of this series was “dismantling systemic oppressions” and “combating social injustice.”
The actual result was a muddled set of platitudes from its speakers that offered minimal, if any, substantive insight into behavioral health.
For example, in a talk titled “Mindful Communities: Rehumanizing Behavioral Health through Community, and Connection,” children’s mental health specialist Neerja Singh suggested that organizations “reduce administrative burdens,” and that policies should be shifted “from top-down mandates to community-driven solutions.”
It sounded promising at first—but what did it actually mean? As the conference went on, attendees were told that the healthcare system is fundamentally unequal, that racism and xenophobia are pervasive and foundational throughout healthcare. No concrete examples were given about reducing administrative burdens, and the so‑called “community‑driven solutions” were framed in the language of identity politics. Far from resembling a localized approach to improving mental health, the conference ultimately came across as a confused mix of bureaucratic social engineering that bordered on incoherence.
To begin, the first speaker presented a slide that, to put it mildly, was baffling in its intent. Titled “System We Work in Based on,” it listed several bullet points that appeared to reflect her perspective on those factors underlying the behavioral health system:
“Philosophy of Othering than Mutuality”
“Oppression on the Name of Equality”
“Dominant Culture is Uncomfortable with Equity”
“Dominant Culture’s Discomfort is Running the System”
Confused grammar and verbiage gave the impression that the presenter might not fully grasp her own message and the content itself seemed disconnected from any meaningful point. It left one wondering: What exactly was she trying to communicate?
What is the current dominant culture, and what exactly is that “discomfort” claimed to be “running the system?” How does one even measure discomfort in this context?
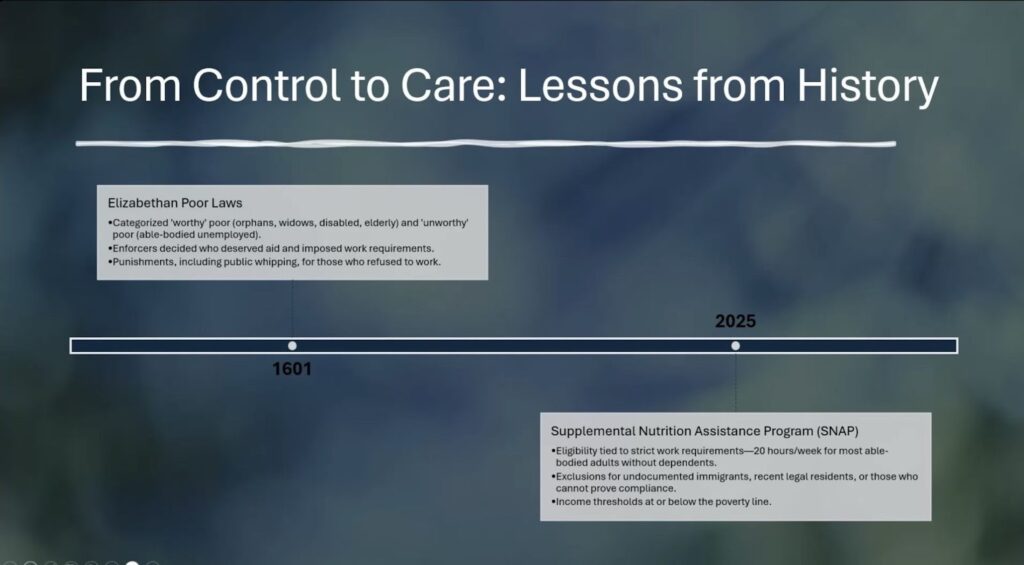
The lack of coherence was made clearer when viewers were introduced to a slide titled “From Control to Care: Lessons from History.”
From UW Medicine’s “Reimaginging Behavioral Health: Race, Equity, & Social Justice Conference” (September 2025).
In this overly simplistic view of our nation’s past, participants were informed of society’s “jump” from an oppressive Elizabethan-era (complete with “public whipping”) to a modern-day utopia that includes the Supplemental Nutrition Assistance Program (SNAP). No explanation was provided for any of it, despite the speaker informing viewers that “knowing this history is essential to dismantle entrenched biases.”
Considering that the presenter is a psychologist and not a historian, her limited and overly simplified portrayal of the past could be forgiven. However, the overall presentation came across as disjointed and lacking in the psychological depth one would expect from a behavioral health conference, leaning heavily on advocacy at the expense of educational content.
As the conference progressed, participants were introduced to numerous unsubstantiated assertions without the backing of evidence.
Following multiple slides about the impact of culture on health, a graphic illustrating “Systemic Inequities & Barriers” declared that problems in healthcare are “not ‘just’ a clinical issue,” but a “social justice issue.”
From UW Medicine’s “Reimaginging Behavioral Health: Race, Equity, & Social Justice Conference” (September 2025).
The continued assertions of “systemic inequities,” as we can see at the top of the slide in bold print, are done without any proof. We’re simply told there is “racism,” “ongoing discrimination,” and the like. Moreover, suggesting that professionals aren’t “culturally competent,” despite the extensive training they receive, is both factually unfounded and unduly disparaging.
Mental health providers dedicate themselves each day to serving people from all backgrounds with compassion and generosity. Their focus is on addressing the behavioral health needs of the individuals they support. They need not become the next social justice warrior, but rather strengthen their expertise and professional skills.
Nevertheless, the perspectives of the speakers—who appear more like activists themselves rather than clinicians—hold significant influence, especially when amplified through the platform of a professional conference. For attendees passionate about the field of behavioral health, such presenters often command considerable authority. This makes it all the more essential that their insights be delivered with nuance and intellectual integrity. When their messaging veers toward ideological persuasion rather than grounded, evidence-based analysis, it becomes a cause for serious concern.
It is either reckless or purposefully misleading.
Sadly, this reflects a troubling trend in the education of healthcare professionals where advocacy has taken the lead at the expense of any intellectual rigor: declare a preferred belief, then reinforce it through repetition until it gains the appearance of truth.
People with professional credentials repeatedly declare that there is structural racism, and to combat it, systems must be dismantled. The reason for restructuring the system is because there is structural racism, which is evidenced only by the fact that they said there is.
It’s a closed loop. It is also why those lecturing at UW Medicine’s conference can bring up ideas like “ethical harm through cultural invalidation” without defining what any of those terms mean. Doing so is an example of indoctrination disguised as legitimate continuing education. We need better for our behavioral health professionals and the individuals they support.
https://donoharmmedicine.org/wp-content/uploads/2024/03/shutterstock_351708407-scaled.jpg17002560Naomi Rischhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngNaomi Risch2025-11-17 16:08:162026-02-11 15:34:15UW School of Medicine: Behavioral Health Education, or Social Justice Indoctrination?