Earlier this month, we lamented the UC Berkeley School of Public Health’s reliance on woke buzzwords and abstractions. A glance at the Yale School of Public Health’s “U.S. Health Justice Concentration” reveals that the problem goes from coast to coast.
Yale SPH introduces its program of study with a number of evidence-free claims:
“Vast, persistent and avoidable health inequalities by race, geography, class, gender identity and sexual orientation are well documented.”
“[S]ystems and processes … perpetuate health injustice in the United States.”
“[P]ast and present systems of privilege and power, related to race, class, gender, sexual orientation and other identities, create unequal burdens on health that are avoidable and unjust.”
There is a kernel of truth in some of these assertions, especially the contention that past racism (e.g., before and during the Civil Rights Era) previously affected health outcomes.
Yet the broader implication — that today’s health “inequalities” are exclusively or primarily the result of oppressive “systems” — begins by disregarding the role that individual behavior plays in patient health.
To name only the most obvious example, smoking, which dramatically increases one’s risk of lung cancer and cardiovascular disease, is not “systemic”; it is personal.
This medical reality seems to be lost on Yale SPH’s curriculum designers. Students pursuing a U.S. Health Justice Concentration must take “SBS 590 Advocacy and Activism,” a course in which they are taught “the theoretical frameworks and the practical applications of community organizing and advocacy as a means of subverting traditional systems of power.”
Among the academic offerings from which they may choose are “SBS 592 Biomedical Justice: Public Health Critiques and Praxis” and “SBS 593 Community-based Participatory Research in Public Health,” classes in which students “analyze and critique public health methodology, discourse, and practice from a health justice framework” and consider “an effective strategy to understanding and addressing health disparities in public health and ultimately achieving health equity,” respectively.
In other words, Yale SPH is interested in producing not public-health experts but professional activists. This is a serious mistake. “Subverting traditional systems of power” may align with ideological goals, but it will do nothing to address the next pandemic.
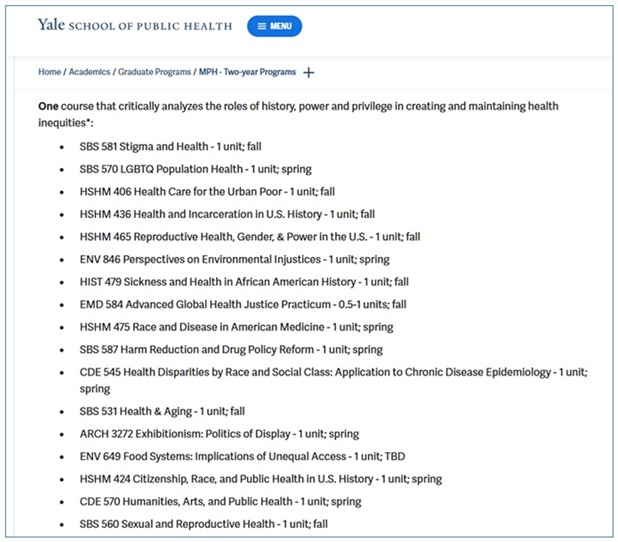
Things get even worse as one moves down the concentration’s page. Students must take one course that “critically analyzes the roles of history, power and privilege in creating and maintaining health inequities.”
They must take another that “discusses how systems of government and law affect health equity at the local, state, and national level.”
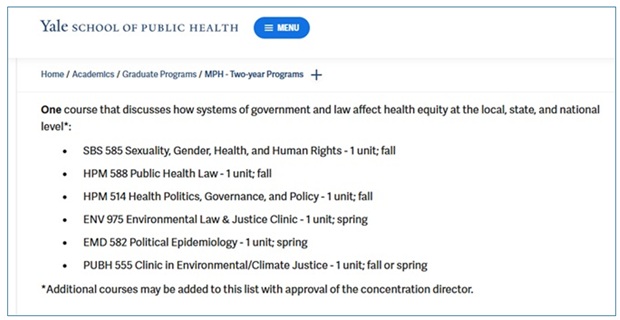
Again, the focus here is on ideological assumptions and agitation. (“EMD 582 Political Epidemiology” is a particularly brazen offender.) Students interested in the fundamentals of public health will need to search outside of this concentration.
Indeed, a look at the U.S. Health Justice Concentration’s student “competencies” list suggests that actual public-health instruction is far from Yale SPH’s mind. Much is made therein of “community organizing,” “power, privilege, and history,” “critical justice,” and “positionality, subjectivity, power and privilege.” Little is made of how diseases spread or how populations adopt healthy behaviors.
As at UC Berkeley, this move away from science and toward political advocacy will please students who see public health as a means to ideological ends. But it may have real health consequences for the rest of us.



