Richmond, VA; December 10, 2024 – Today, Do No Harm released a new report exposing the role of the Association of American Medical Colleges (AAMC) in politicizing the nation’s medical schools.
The report, titled, “Activism Over Meritocracy: How the Association of American Medical Colleges is Corrupting Medical Education with Endless DEI Ideology,” is broken into the three parts:
Part One outlines how the AAMC pressures medical schools and residency programs to impose DEI ideology on students and applicants.
Part Two reveals how the AAMC engages in expensive lobbying efforts and political activism to advance its agenda.
Part Three proposes strategies for countering the well-entrenched DEI agenda that the AAMC has inflicted upon the American medical education system.
“The AAMC corrupts medical education by blatantly embedding DEI into American medical schools,” said Dr. Jared Ross, Senior Fellow at Do No Harm. “Our report offers practical solutions to restore excellence in the medical school curriculum. The medical education system in this country should be focused on science-based teachings rather than forcing students to engage with a radical political ideology.”
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. With 14,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 14 countries, DNH has achieved over 10,000 media hits in top-tier publications and garnered widespread attention through numerous broadcast news appearances.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2024-12-10 12:19:332026-02-11 15:33:55Do No Harm Releases New Report Exposing the Association of American Medical Colleges for Politicizing Medical Education
The University of Vermont Larner College of Medicine discontinued its discriminatory Visiting Student Elective Scholarship Program (VSESP) following a Do No Harm federal civil rights complaint filed against the school.
The program was a four-week clerkship for emergency medicine medical students and included a $2,500 stipend for travel and housing costs. The original eligibility requirements stated that applicants should “describe how you identify as one or more of the Larner College of Medicine’s diversity categories (such as Black/African American, Hispanic/Latino, Native American, Pacific Islander, or low socioeconomic status).”
In other words, the scholarship effectively excluded students who were white, Asian, Middle Eastern, and from other unfavored racial groups.
Additionally, the scholarship’s description stated that its purpose was to “provide mentorship and networking for fourth-year medical students underrepresented in medicine such as racial and ethnic minorities, LGBTQ-identified or gender nonconforming individuals.”
The requirements, in short, amounted to explicit and unlawful racial discrimination in clear violation of federal civil rights laws.
Do No Harm Senior Fellow Mark J. Perry filed a federal complaint against the university with the Department of Education’s Office for Civil Rights (OCR) in November 2023 and sent a copy courtesy of the complaint to several of the university’s leaders, including the General Counsel and President. The complaint alleged the university violated federal civil rights protections under Title VI and Title IX.
By May of 2024, the university had removed the discriminatory eligibility criteria for the program and replaced it with a brief blurb on the program’s selection criteria.
“Successful applicants will be those who are able to demonstrate their commitment to the Larner College of Medicine’s Tenets of Professionalism and how their unique lived experience will advance diversity, equity, and inclusion in medicine and improve health care delivery to underserved areas and populations,” the updated description read.
However, it now appears that the discriminatory program has been discontinued altogether, as the link to the scholarship program has not been active since July. Rather than a specific VSESP program for emergency medicine students, there is now a general scholarship program for all medical students that does not include discriminatory eligibility requirements.
“OCR determined that the University currently advertises VSESP on this website, which does not indicate any restriction or preference based on race, color, national origin, or sexual orientation,” OCR wrote in a letter to Do No Harm.
“Based on this information, OCR has determined that the facts underlying the allegations of race, color, national origin, and sexual orientation discrimination are no longer present and OCR has no evidence that the law is violated,” the letter reads.
This OCR ruling is a welcome victory for all of the students who have been denied educational opportunities due to the University of Vermont’s unlawful discriminatory eligibility criteria. Moreover, it’s a welcome sign that the University of Vermont realized the error of its ways and took corrective action to comply with federal civil rights laws in response to Do No Harm’s complaint.
Have you been unfairly affected by discriminatory scholarships or programs at your institution, or are you aware of any discrimination at a U.S. medical school? If you or others did not apply because you thought you were ineligible, please let us know – anonymously and securely.
https://donoharmmedicine.org/wp-content/uploads/2023/12/shutterstock_2363563829-scaled.jpg17092560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2024-12-09 17:30:532026-02-11 15:33:55Vermont Med School Discontinues Racially Discriminatory Program After Do No Harm Complaint
Would you want your hospital inculcating staff members on the benefits of racially discriminatory policies?
Do No Harm obtained video recordings of four virtual trainings held for staff members at University Hospitals of Cleveland this summer. The trainings featured discussions on topics such as implicit bias that are staples of DEI discussions.
But one particular training, featuring Cleveland’s Director of Public Health David Margolius, extolled the virtues of racial reparations, with Margolius recommending reparations as a way of closing the racial gap in health outcomes.
“The problems that we’re facing all stem from the wealth gap between predominantly white families and predominantly black families,” he said, referencing a talk he gave in 2023 that explored his reparations activism in greater detail. “So, the way to fix that is reparations.”
“Ultimately, if we want to directly address this [disparity], it’s reparations,” he added.
Additionally, in the 2023 talk, Margolius argued the best way to sell reparations to the public (who by and large are not fans of racially discriminatory policies) is to frame it as a “public health intervention.”
“I think we need to continue to communicate it as a public health intervention to make it more mainstream,” he said.
Ideastream Public Media reported in August 2023 that Margolius would continue to advocate for reparations.
“It’s a proven public health intervention that we should continue to advocate for on a national level,” he said.
Figure 1. Screenshot from the University Hospitals training.
A more cynical viewer might interpret Margolius’ comments as smuggling an unpopular political agenda into the mainstream through a more socially-acceptable veneer.
This is part of a larger issue in the healthcare field, especially among medical associations and educational institutions, in which the lines between “health” and “politics” are increasingly blurred. Do No Harm’s latest research project, Outside Their Lane: Mission Creep in Medical Specialty Societies, demonstrated how medical specialty societies use their expertise to take positions on hot-button social and political issues, often cloaking their activism under the guise of advocacy for “public health.”
This training is in a similar vein: openly pushing a particular public policy prescription (that happens to be racially discriminatory, for what it’s worth) under the guise of public health education.
Regardless of whether these arguments have merit, they belong in the political sphere.
DEI trainings, especially in the public health sector, have always been thinly-veiled excuses to platform a political agenda.
University Hospitals should reconsider its priorities and abandon DEI: the medical field deserves better.
https://donoharmmedicine.org/wp-content/uploads/2023/09/shutterstock_165320348-scaled.jpg16962560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2024-12-09 15:32:212026-02-11 15:33:55University Hospitals of Cleveland Pushes ‘Reparations’ in DEI Trainings
On Wednesday, as the Supreme Court heard oral arguments in a case pivotal to future efforts to restrict child sex change interventions, Do No Harm hosted our “Stop the Harm” rally featuring prominent voices advocating against these dangerous practices.
The event was an enormous success, even going viral on social media, as crowds of Americans gathered to cheer on our cause and the importance of protecting our country’s children. Advocates, lawmakers, and physicians alike all joined together to explain why the Supreme Court must uphold prohibitions on child sex change interventions.
Detransitioner @ChoooCole: “We need to fight for our children and families!!” pic.twitter.com/lbtcYwH5eG
Figure 1. Do No Harm External Relations Manager Beth Serio speaks at the Stop the Harm rally.
Hosted by our own Beth Serio, the rally’s speakers included the Daily Wire’s Matt Walsh, the American Principles Project’s Terry Schilling, and representatives from over a dozen other organizations such as the Alliance Defending Freedom.
Do No Harm was also joined by Tennessee lawmakers William Lamberth and Jack Johnson, who were behind the Tennessee law restricting child sex change interventions at the center of the Supreme Court case. Moreover, the rally featured members of Congress including Rep. Marjorie Taylor Greene (R-GA) and Rep. Gary Palmer (R-AL), and Do No Harm staff, fellows, and advocates.
Here’s my speech outside SCOTUS. As expected the trans activists tried to sabotage us by being loud and obnoxious. That’s all they can do now. They’re losing on every front. They can only scream impotently into the void while we burn their ideology to the ground. Fine with me. pic.twitter.com/ZU9Xj0oxRj
The case in question, United States v. Skrmetti, concerns a Tennessee law prohibiting doctors from performing so-called “gender-affirming care” on children. This includes cross-sex hormones, puberty blockers, and surgical procedures.
Figure 2. Matt Walsh speaks at the Stop the Harm rally.
The ACLU first sued Tennessee over the law, and the Department of Justice under President Joe Biden intervened in the case in 2023, arguing the law violated the Equal Protection Clause of the Fourteenth Amendment. Seeing as 26 states including Tennessee have passed laws restricting child sex change interventions, the Supreme Court’s decision in this case will likely have wide-reaching consequences for the protection of children across the country.
“I’m confident that the highest court in our land will stand for not only what is morally and ethically right, but with the scientific and medical literature, and ban the medical and surgical experimentation on innocent children once and for all,” said Do No Harm Senior Fellow Dr. Jared Ross.
Tennessee lawmakers William Lamberth and Jack Johnson, who are behind the bill at the heart of today’s Supreme Court case, speak outside the court after oral arguments. @DailyCallerpic.twitter.com/axy3SLopRC
“The most central and fundamental duty of any society is to protect their children,” said the Daily Wire’s Matt Walsh. “Children are innocent and helpless. They know very little about themselves and very little about the world around them. They rely on us for clarity and guidance … they trust us adults implicitly.”
“If we will not fulfill that obligation then we are worse than useless,” he continued.
Do No Harm Parent Advocate January Littlejohn shared her own harrowing experience with her thirteen year-old daughter.
Figure 3. Do No Harm Parent Advocate January Littlejohn speaks at the Stop the Harm rally.
“Our daughter at thirteen was encouraged through activism and peer pressure to disassociate from her body and to believe her body parts could simply be removed, modified or replace,” Littlejohn said. “She cavalierly talked about getting puberty blockers and getting a double mastectomy, that has been rebranded as ‘top surgery.’ But it was clear to us she did not understand the gravity or scope of what she was requesting.”
Pro- children advocates blast “Proud To Be An American,” drowning out the pro-transgender activists pic.twitter.com/SNMHvIIz7k
Her thoughts were echoed by American Principles Project President Terry Schilling.
“I have a very simple message to the trans industry: You will not take our children,” Schilling said. “And your days of harming [other] children are numbered.”
My hit on Fox today about the SCOTUS Skrmetti case.
Figs. 4-5. Do No Harm Patient Advocate Chloe Cole speaks at the Stop the Harm rally.Figure 6. Do No Harm Parent Advocate January Littlejohn speaks with a reporter during the Stop the Harm rally.
Inside the courthouse, the majority of the justices were skeptical of the federal government’s arguments and of the efficacy of so-called “gender-affirming care” more broadly, with many of them bringing up evidence that
“It strikes me as a pretty heavy yellow light, if not red light, for this court to come in, the nine of us, and to constitutionalize the whole area, when the rest of the world, or at least the people who the countries that have been at the forefront of this, are pumping the brakes on this kind of treatment,” said Justice Brett Kavanaugh.
“Why isn’t it best to leave it to the democratic process?” Kavanaugh asked at another point.
Justice Samuel Alito cited the Cass Report, a nearly 400-page report that examined “gender identity services for children and young people” in the United Kingdom. The report, which was commissioned by the National Health Service (NHS) England roughly four years ago, found “remarkably weak evidence” to support the use of puberty blockers and hormone treatments for gender distressed children.
Alito brought attention to a particular passage that found no evidence child sex change interventions reduced suicides in gender distressed youth. ACLU lawyer Chase Strangio admitted that this was the case.
Huge moment at SCOTUS. Alito pulled up Page 195 of the Cass report, showing that child sex-changes don't actually prevent suicide. ACLU attorney Chase Strangio admits in response that there's "no evidence" that these procedures actually reduce suicides.
Chief Justice John Roberts noted that the lack of evidence for these practices made it all the more reasonable to allow states to restrict them.
“Doesn’t that make a stronger case for us to leave those determinations to the legislative bodies rather than trying to determine them for ourselves?” he said.
However, not all the justices appeared to quite understand the gravity of what was at stake, or the serious harms of these medical interventions.
Rice: "How many minors have to have their bodies irreparably harmed for unproven benefits?"
For instance, Justice Sonya Sotomayor trivialized the harms of child gender medical interventions by stating that every medical procedure carries some degree of risk, bringing up the example of taking an “aspirin.”
This line of reasoning fails to acknowledge that there are medical procedures with high risks and uncertain to nonexistent benefits (like, say, gender medical interventions), and it would be grossly irresponsible for a physician to perform such procedures in almost any other scenario.
Nevertheless, the outpouring of support evident at the rally today only reinforces the empirical reality that the public is on our side. Americans do not want their children subjected to dangerous and unproven medical interventions in service of radical gender ideology. Laws prohibiting these practices are essential to protect this country’s youth.
We hope the Supreme Court agrees.
https://donoharmmedicine.org/wp-content/uploads/2024/12/unnamed-2.jpg16001200Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2024-12-04 20:33:302026-02-11 15:33:55Do No Harm Hosts ‘Stop the Harm’ Rally on Steps of Supreme Court
In this thought-provoking episode of the Do No Harm Podcast, hosts Ian Kingsbury and Scott Centorino are joined by college student and former transgender individual, Simon Amaya Price, to explore the complex intersection of politics, medicine, and gender ideology. Simon shares his personal story of de-transitioning, the challenges he faced as an outspoken critic of gender affirming care, and the controversy surrounding his attempt to host a campus event on this topic.
The conversation dives deep into the political and scientific tensions around gender dysphoria, the role of diversity and inclusion in academic settings, and the experiences of de-transitioners who often face opposition on all sides. Gain unique insight into the narratives left unheard, the role of activism in shaping public discourse, and why protecting free speech and medical integrity is more crucial than ever. You won’t want to miss this candid and compelling discussion.
This video contains graphic medical content that some viewers may find disturbing. Viewer discretion is advised.
https://donoharmmedicine.org/wp-content/uploads/2024/12/Do-No-Harm-Podcast-S3-EP11-SIMON-AMAYA-PRICE-scaled.jpg14402560rededge-rachelhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngrededge-rachel2024-12-03 22:11:562026-02-11 15:33:55S3E11: Examining Gender Ideology and Free Speech with Simon Amaya Price
Richmond, VA; November 27, 2024 – The Centers for Medicare and Medicaid Services (CMS) announced a new rule intended to increase access to kidney transplants. The finalized rule dropped a proposed requirement for hospitals to submit “health equity plans” to receive incentive payments. The change comes after Do No Harm submitted a comment on the original rule stating that the health equity plan requirement would have encouraged race-based discrimination.
“Racial discrimination has no place in healthcare,” said Dr. Stanley Goldfarb, Chairman of Do No Harm. “Had the rule taken effect as proposed, the government would have been putting its thumb on the scale by incentivizing providers to consider race when selecting patients for kidney transplants. We are pleased the CMS took our concerns seriously and made the necessary adjustments to the final rule.”
Furthermore, after consideration of the public comments we received, we will not be finalizing a health equity performance adjustment provision, as described in section III.C.5.c(3) of this final rule. Therefore, we are modifying regulatory text for the achievement domain definition at § 512.402, to remove references to a health equity performance adjustment and make minor technical corrections in punctuation.
Last month, Do No Harm releaseda continuing medical education course that examines the impact of considering race in kidney disease assessments. Click here to take the free course.
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. With 14,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 14 countries, DNH has achieved over 10,000 media hits in top-tier publications and garnered widespread attention through numerous broadcast news appearances.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2024-11-27 21:07:162026-02-11 15:33:55CMS Removes Equity Requirement from Kidney Transplant Rule Following Do No Harm Comment
We at Do No Harm have long been sounding the alarm over the deleterious effects of DEI training, particularly in the field of medicine where lives are literally at stake. DEI is a radical ideology that encourages hate, divisiveness, and prejudice, the very things its proponents purport to oppose.
Well, a new study found exactly that, and then some.
“Instructing Animosity: How DEI Pedagogy Produces the Hostile Attribution Bias,” released by the Network Contagion Research Institute (NCRI) and the Rutgers University Social Perception Lab on Monday, found that exposure to DEI trainings increased agreement with rhetoric from Adolf Hitler and had a greater desire to punish those they perceived as harboring prejudice, even when none existed.
That’s hardly a ringing endorsement for the DEI project.
The study examined the impact of DEI narratives on participants’ responses on three subjects –race, religion, and caste. The control group was exposed to a neutral essay about corn, while each other group was exposed to various DEI narratives pertaining to each of the subjects. Then, each grouping was presented with a hypothetical scenario and asked questions about their subject.
“Across all groupings, instead of reducing bias, [DEI materials] engendered a hostile attribution bias [ ], amplifying perceptions of prejudicial hostility where none was present, and punitive responses to the imaginary prejudice,” the study found. “These results highlight the complex and often counterproductive impacts of pedagogical elements and themes prevalent in mainstream DEI training.”
The results were particularly disturbing for participants exposed to DEI narratives about the Hindu caste system. DEI materials increased participants’ agreement with quotes from Adolf Hitler in which the word “Jew” was replaced with “Brahmin,” the highest caste.
“Participants exposed to the DEI content were markedly more likely to endorse Hitler’s demonization statements, agreeing that Brahmins are ‘parasites’ (+35.4%), ‘viruses’ (+33.8%), and ‘the devil personified’ (+27.1%),” the study found. “These findings suggest that exposure to anti-oppressive narratives can increase the endorsement of the type of demonization and scapegoating characteristic of authoritarianism.”
Participants exposed to DEI narratives about race read materials from Ibram X. Kendi and Robin DiAngelo, two “scholars” whose “work” is closer to a barely-coherent ideological pretext for racial discrimination and divisiveness. Shockingly, the study found that participants exposed to these materials were considerably more likely to find racial prejudice when none existed, and were more likely to support punishment of the “racist” actor.
But it seems that these damning findings may have been a little too over the target.
National Review reported that editors at both Bloomberg and The New York Times elected to kill stories about the study after reporters had previously agreed to cover it.
“Unfortunately, both publications jumped on the story enthusiastically only for it to be inexplicably pulled at the highest editorial levels,” a NCRI researcher told National Review. “This has never happened to the NCRI in its 5 year history.”
Bloomberg failed to provide an explanation, while some inside The New York Times had concerns the research was not peer reviewed.
“I told my editor I thought if we were going to write a story casting serious doubts on the efficacy of the work of two of the country’s most prominent DEI scholars, the case against them has to be as strong as possible,” a New York Times reporter wrote to the NCRI, per National Review.
It’s a shame these publications refused to run these stories so that this research could not reach a wider audience. The study highlights the dangers of DEI in the medical field and why it is absolutely imperative that healthcare professionals don’t simply turn a blind eye to these practices, but actively resist.
Engendering racial paranoia and encouraging physicians to find prejudice under every bed is a recipe for disaster. And in the medical field, where patients are trusting healthcare professionals with their lives, it is completely unacceptable to subject these doctors and nurses to propaganda that encourages authoritarian, prejudicial impulses.
https://donoharmmedicine.org/wp-content/uploads/2024/11/shutterstock_1754251778-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2024-11-25 21:24:092026-02-11 15:33:55Study Finds DEI Training Increases Agreement With Hitler’s Rhetoric – And the Media Won’t Touch It
A look around the political and corporate landscape reveals that DEI is in retreat. Its champions are trying to salvage it with claims that it’s beneficial, but they remain as wrong as ever.
Take, for example, an article published November 11 in STAT News called Cardiovascular health disparities persist in puzzling ways, studies find. The author admits that DEI is facing “political winds” but insists that four recent studies demonstrate why DEI is supposedly beneficial. Closer inspection reveals this assertion to be false.
The first “study” mentioned in the STAT News article is called “Relationship Between Race, Predelivery Cardiology Care and Cardiovascular Outcomes in Pre-Eclampsia/Eclampsia Among a Commercially Insured Population.” The researchers observe that among white mothers with eclampsia or preeclampsia (dangerous hypertensive pregnancy disorders), receipt of predelivery cardiology care is associated with a lower incidence of major adverse cardiovascular events, or MACE (a composite measure of heart failure, acute myocardial infarction, stroke, or death). However, for black mothers with eclampsia or preeclampsia, receipt of cardiology care is not associated with a lower incidence of MACE.
In making sense of the different outcomes, the researchers couch their explanation in default DEI positions, blaming “structural racism” and “racial biases in the delivery of appropriate and timely post-partum cardiology care.” As is so often the case with health disparities, a closer look reveals less interesting but more sensible explanations.
One plausible explanation for the disparity is that preeclampsia is “more severe in women with African ancestry.” Likely, black women with preeclampsia who receive cardiology care have worse outcomes because they have more severe disease. The researchers theoretically address this concern by statistically adjusting their estimates to account for differences in preexisting heart conditions (cardiac dysrhythmia, valvular heart diseases, ischemic heart diseases, cardiomyopathies, and heart failure) and clinical morbidities (e.g. diabetes, assisted reproductive technology, dyslipidemia, hypertension, gestational hypertension, stroke, obesity, and obesity in pregnancy). However, this data does not perfectly capture differences in health across populations, and these differences can matter when interpreting results. A study purporting to show that black babies were less likely to die if assigned to black doctors was recently debunked by the discovery that researchers did not account for differences in the incidence of “very low birth weight.” In a similar vein, controlling for “obesity” masks significant racial differences in the incidence of morbid/clinically severe obesity.
Another factor that plausibly explains the phenomena observed by the researchers is average group differences in how patients interact with the health care system. Black women are more than twice as likely as white women to receive late or no prenatal care. Likely, many who receive delayed care would have received an earlier referral to cardiology and better outcomes if they had secured timely care. In writing about limitations, the researchers correctly note that “we were unable to ascertain the frequency and timing of cardiology care throughout the pregnancy period. We appreciate that these factors may have [a] substantial impact on the care and outcomes for both races.” Nevertheless, this possibility is eschewed in favor of a radical, racialized hypothesis.
The second “study” in the STAT News article is called “Racial and Ethnic Differences in Semaglutide Prescriptions for Veterans with Overweight or Obesity in the Veterans Affairs Healthcare System.” The researchers observe that black veterans in the VA health system are marginally less likely to be prescribed semaglutide as a treatment for obesity (8.9% for black veterans vs. 9.1% for white veterans). As the authors reasonably argue, the small difference masks the true magnitude of the disparity since black patients are, on average, in greater clinical need of weight loss treatment.
What the researchers get wrong is asserting “structural bias” as a plausible explanation for the disparity. The idea that structural bias permeates the healthcare system is born of the fallacious ideas that group differences are indicators of maltreatment and that the pseudoscience of “implicit bias” provides meaningful insight into American healthcare. Likely, the lower receipt of semaglutide simply reflects average group differences in demand for treatment or treatment hesitancy.
Not only is the assertion about “structural bias” wrong, it is also logically inconsistent. The next study highlighted by STAT News is called “Social Determinants of Health and Disparities in Guideline-Directed Medical Therapy Optimization for Heart Failure.” According to that study, black and Hispanic patients with heart failure with reduced ejection fraction (HFrEF) are more likely than white patients with the same condition to receive quadruple therapy optimization, the optimal treatment plan for that condition. According to the logic that disparities that disadvantage a group are evidence of maltreatment against that group, the findings would suggest – absurdly – that “structural bias” in healthcare exists against white patients. In reality, disparities that at times favor one group and at other times favor a different group reveals the complex, multifaceted nature of health disparities as well as the absurdity of DEI orthodoxy and its default explanation of racism.
The final study cited by STAT News is called “Perceptions About Diversity, Equity, and Inclusion Among Cardiovascular Fellows‐in‐Training.” The “researchers” observe that some of the cardiovascular fellows-in-training who answered their survey feel that DEI efforts in their programs are insufficient. For example, “Although 66% felt DEI was an institutional priority and 63% a fellowship priority, 34% of participants strongly or somewhat agreed that community engagement and outreach was not valued by their institution.” The trouble is that the efficacy and wisdom of DEI aren’t ultimately determined by the sentiment of a small group of activist physicians but by how DEI impacts medicaleducation and patient outcomes. The verdict couldn’t be clearer.
https://donoharmmedicine.org/wp-content/uploads/2024/11/shutterstock_2481473875-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2024-11-21 15:27:312026-02-11 15:33:54Activists Trot Out Bogus Studies to Defend DEI in Medicine
Following the “racial reckoning” of 2020, numerous medical associations and specialty societies took it upon themselves to delve into the realm of political and racial activism, promoting DEI and radical ideology to the detriment of medical education and, ultimately, patients themselves. This is a phenomenon that Do No Harm has extensively recorded.
These efforts often manifested in projects intended to rewire the landscape of medicine through trainings and continuing education that pushed the precepts of DEI onto the healthcare system.
Take the Alliance for Academic Internal Medicine (AAIM). This is the fourth year that AAIM will be offering its $400,000 grant program, “Building Trust through Diversity, Health Care Equity, Inclusion and Diagnostic Excellence in Internal Medicine Training.”
We don’t have to speculate about whether the grant program is intended to reform medical education in accordance with a radical ideology; AAIM literally says that’s the case. The purpose of the funds, per AAIM, is to “integrate diversity, equity, and inclusion (DEI) into the fabric of internal medicine education and training.”
In fact, the inaugural grant announcement contained this same language. It further noted that “bias and discrimination in health care have slowly but steadily eroded trust in the entire system, including in clinicians directly responsible for care.” (We agree! Although not for the same reasons as AAIM).
The grant program specifically courts applications to develop “training programs that incorporate DEI, and in particular those that employ inter-professional education best practices.”
One previous grant recipient aimed to “expand the curriculum for primary care residents to include education about […] patient mistrust and physician bias.” And to illustrate just how tied this program is with political activism, a 2023 grant recipient received $40,000 for a project titled “Integration of Voter Registration within a Safety-Net Health System to Address Voting as a Social Determinant of Health.”
AAIM even appears to invite applications to develop newfangled methods for racial discrimination, asking for “approaches that foster and support diverse and equitable pathways into medicine and faculty and leadership positions.”
But what makes this program particularly problematic is the fact that AAIM is composed of several organizations that represent not just medical providers or students but the educational decision-makers. These include department chairs of internal medicine at medical schools, fellowship program directors, residency program directors, and more.
In other words, AAIM represents the standard-setting movers and shakers in internal medicine education. And its focus is to propagate DEI throughout the field of academic internal medicine and in its own words, integrate DEI into internal medicine’s fabric.
Let’s not sugarcoat it: This is a full-fledged ideological assault intended to remake medicine into a new, DEI-centric discipline that prioritizes activism and supports racial discrimination to achieve its “equity” goals.
The physicians of tomorrow should not be ideologues. And AAIM should take its responsibility more seriously and commit to excellence, not “equity.”
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_1994910104-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2024-11-21 13:52:512026-02-11 15:33:54The $400,000 DEI Program to Turn Internal Medicine Inside-Out
In this episode of the Do No Harm podcast, host Ian Kingsbury welcomes Representative Jeremy Faison, a Republican member of the Tennessee House of Representatives. Join them as they delve into Faison’s unique political journey from pest control business owner to state legislator. Discover how he navigates the challenges of balancing public service with his entrepreneurial endeavors. Faison shares his candid views on diversity, equity, and inclusion (DEI) and its impact on identity politics and systemic racism. Gain insights into the legislative process in Tennessee and Faison’s commitment to representing his constituents while staying true to his values. Tune in for an engaging discussion that highlights the intersection of personal conviction and public duty in today’s political landscape.
https://donoharmmedicine.org/wp-content/uploads/2024/11/Do-No-Harm-Podcast-S3-EP10-REP-FAISON-scaled.jpg14402560rededge-rachelhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngrededge-rachel2024-11-20 18:11:332026-02-11 15:33:54S3E10: Balancing Bugs and Bills: A Conversation with Representative Jeremy Faison
Medical specialty societies, like the American Academy of Pediatrics, are key players in American healthcare and are responsible for developing clinical guidelines and providing continuing medical education. But according to Do No Harm’s report, these organizations routinely participate in political advocacy on topics unrelated to medicine.
The report tracks the medical societies’ official public stances on hot-button issues including affirmative action/racism, climate change, the Russian invasion of Ukraine, immigration policy, and conflict between Israel and Hamas. Since 2010, 93% of specialty societies published statements on affirmative action or racism, 57% on climate change, 50% on immigration, 39% on Ukraine, and 18% on the ongoing war in the Middle East.
“The politicization of medical societies represents a betrayal of the public’s trust in healthcare,” said Do No Harm Chairman Dr. Stanley Goldfarb. “Dues-paying members of the societies and the public they serve should expect nothing less than institutional neutrality from all specialist groups.”
To track the societies’ politicization, Do No Harm identified 28 core medical specialties and then identified the related medical associations. Do No Harm then searched the organizations’ websites for official statements, such as press releases, open letters, or position statements published in academic journals, on political issues and events.
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. With 14,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 14 countries, DNH has achieved over 10,000 media hits in top-tier publications and garnered widespread attention through numerous broadcast news appearances.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2024-11-20 14:24:062026-02-11 15:33:54New Do No Harm Report Exposes Increasing Politicization of Medical Establishment
Americans are becoming more and more in favor of restricting child sex change interventions, according to a poll released Monday.
The poll, released by Napolitan News Service and conducted by RMG Research, found that 72% of Americans believe it should be against the law to provide “children under 18 with puberty blockers, drugs, and/or surgery to help them transition from one gender to another,” with just 18% saying the interventions should be legal.
This is a marked increase from just a few months ago; in August, only 62% of Americans supported banning child sex change interventions, and 24% supported their legality, according to the poll.
Should it be against the law to provide children under 18 with puberty blockers, drugs, and/or surgery to help them transition from one gender to another?
What’s more, it coincides with heightened attention to and awareness of the child sex change issue and gender ideology more broadly. In October, Do No Harm launched our Stop the Harm database that catalogs child sex change interventions performed by hospitals around the country.
We’ve been working tirelessly to bring attention to the dangers posed by these experimental and unsupported medical procedures, and it looks like the public is increasingly catching on.
States have in turn sought to crack down on child sex change procedures, with 26 states passing laws restricting so-called “gender-affirming care” for children.
The poll also asked respondents if teachers and schools should be required to notify a student’s parents if the student wants to change his or her gender, name, and pronouns. A vast majority said “yes” at 73%, while only 17% said “no.”
The poll surveyed 1,000 registered voters online on November 13 and was conducted by Scott Rasmussen, president of RMG Research. The margin of error is plus or minus 3.1%.
https://donoharmmedicine.org/wp-content/uploads/2023/05/shutterstock_526407691-scaled.jpg15902560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2024-11-18 22:15:282026-02-11 15:33:54Americans Increasingly Back Restrictions On Child Sex Change Procedures
The Association of American Medical Colleges (AAMC) has long been a proponent of so-called “holistic review” medical school admissions that devalue test scores and grades to make room for other, less merit-based factors. This approach is often justified on the grounds of pursuing “equity,” and holistic review can be an end-around for race-based admissions.
In its 2024 report on how to interpret MCAT scores, the AAMC argues that admissions officers should take into account students’ “educational opportunities, lived experiences, attributes, and other factors” to demonstrate their commitment to “equity in medical education.”
Buttressing this argument is the following claim:
“Research suggests the differences in MCAT scores for examinees from groups underrepresented in medicine based on race/ethnicity and other background characteristics reflect societal inequalities in income, education, and other factors rather than test bias,” the report reads.
To support this claim, the AAMC cites a 2013 article co-authored by two AAMC officials and published in the AAMC’s journal, Academic Medicine, that identifies several studies finding socioeconomic disparities between racial groups and linking these disparities to gaps in academic achievement.
There is, of course, a credible element to this statement: that students with higher socioeconomic status may have better MCAT scores due to better access to academic resources (e.g. MCAT tutoring) and the ability to afford the opportunity cost of studying.
But coupled with the AAMC’s recent defense of explicit race-based admissions (and current support of “holistic review” admissions that are often a proxy for considering applicants’ race), the implication is clear: MCAT scores should be weighted differently depending on the applicant’s race.
In fact, elsewhere in the report, the AAMC cites a 2020 article published in Academic Medicine called “The Consequences of Structural Racism on MCAT Scores and Medical School Admissions: The Past Is Prologue.” That article’s authors were Drs. Catherine R. Lucey and Aaron Saguil, who chairedthe AAMC’s MCAT Validity Committee and provided recommendations for broadening access to medical education. The article argues that “equitable interpretation of MCAT scores requires consideration of the context in which each applicant earned those scores, rather than assuming that all applicants had equal opportunities.”
There’s a few problems with the AAMC’s approach and its underlying premises.
First, the argument for devaluing MCAT scores relies on the aforementioned claim that racial disparities in MCAT scores can be explained by disparities in socioeconomic status and opportunity.
Figure 1. A chart from the AAMC on the correlation of MCAT scores and academic performance.
However, as the AAMC itself notes in a 2024 report, MCAT scores predict students’ performance better than undergraduate GPAs and, when coupled with GPAs, are the best predictor of student success. In particular, there is a strong correlation between MCAT scores and clerkship or “shelf” exams, as well as United States Medical Licensing Examination (USMLE) clinical knowledge exams.
This means that, in general, the better a student’s MCAT scores, the better they will perform in medical school and the more mastery of clinical knowledge they will exhibit. In short, students with better MCAT scores tend to be better medical students. While it’s certainly possible that, because of socioeconomic hardships, a student scores poorly on their MCAT and then goes on to be an excellent student, this is most definitely not the general trend.
Crucially, this trend cuts against the AAMC’s core argument, and instead indicates that disparities in MCAT scores simply reflect disparities in merit. At a certain point, a student’s academic performance is just reflective of their competence. If the AAMC wants to argue that disparities in competence are due to socioeconomic factors, so be it, but that does not support its argument for devaluing scores.
Second, even if we were to grant the AAMC’s premise, its conclusion and prescription is bizarre. Why should we just consider previous instances of racism when weighting students’ scores? Why not factor in the litany of other historical injustices that may have had cascading effects on the fortunes of today’s prospective medical students? Why not weight scores by parent income, or by whether or not the student grew up in a single-parent household, or whether their community had a public library?
Taking the AAMC’s argument to its logical conclusion reveals how unfeasible and absurd it is. There is no way to properly curve applicants’ scores in an “equitable” manner, and if fairness is the desired outcome, there’s no reason other than racism to make applicants’ race the determinative factor.
Third, the Supreme Court just ruled that race-conscious admissions are illegal. Considering the context in which a student obtained their scores by considering their race is just race-conscious admissions with added steps. And, as Do No Harm has documented, the use of “holistic review” in admissions is a common end-around employed by medical schools to avoid explicitly acknowledging that they are considering applicants’ race.
Undergirding all of this is the fact that the AAMC fundamentally misunderstands the role of the doctor and, by extension, the role of medical schools. The AAMC believes that medical school admissions should be used to redress past racial discrimination, and aims to accomplish this by devaluing the metrics that best reflect and predict merit and competency. But by lowering standards to permit less qualified people to receive a medical education and become doctors, the AAMC is in turn victimizing all patients who are subjected to a lower standard of medical care.
No one deserves to become a doctor. And though the echoes of historical racism may be felt by minority groups today, their situation does not justify further injustices that harm all Americans who enjoy our healthcare system.
Rather than pursuing ideological agendas and manipulating medical schools’ racial composition through holistic reviews, the AAMC should instead commit to prioritizing merit. The most talented applicants should be rewarded.
It’s of critical importance that our country’s future healthcare professionals are the best and brightest. There is very little margin for error.
https://donoharmmedicine.org/wp-content/uploads/2024/11/shutterstock_2479568385-scaled.jpg14402560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2024-11-15 20:51:572026-02-11 15:33:54Equity Over Exams: Why the AAMC’s Arguments for Devaluing Test Scores Don’t Add Up
The Alliance for Regenerative Medicine (ARM), a medical organization focused on cell and gene therapies, removed a race requirement from its GROW RegenMed Internship program after Do No Harm filed a charge with the U.S. Equal Employment Opportunity Commission (EEOC). The program offered students paid summer internship opportunities in the regenerative medicine sector.
Previously, ARM’s internship program was only open to black students.
In July, Do No Harm asked the EEOC to investigate ARM for violating Title VII of the Civil Rights Act of 1964, which prohibits race discrimination in employment. Now, ARM will open the internship to everyone regardless of race.
“Do No Harm welcomes this change,” said Do No Harm Executive Director Kristina Rasmussen. “No student should be denied access to a valuable opportunity because of their race. The medical field is best served when organizations reward students based on their talent and acumen, not traits that have no bearing on their success.”
The change is just the latest example of medical institutions ditching racially exclusionary program requirements following Do No Harm complaints.
For instance, earlier this year, the American Society of Hematology (ASH) rebranded its Minority Recruitment Initiative, a program that awarded scholarships to medical students and residents – but only if they were members of certain “underrepresented” racial groups. The new version of the program, the Hematology Inclusion Pathway (HIP) Initiative, no longer includes language explicitly excluding applicants from certain races. ASH made this change following a series of Do No Harm complaints to the Department of Education’s Office for Civil Rights (OCR) that alleged public universities promoting the scholarship were violating federal civil rights law.
Last month, several medical schools informed the OCR they were either dropping discriminatory eligibility criteria from scholarship programs – or discontinuing the programs altogether – following our civil rights complaints.
https://donoharmmedicine.org/wp-content/uploads/2022/04/shutterstock_89254516-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2024-11-14 13:02:532026-02-11 15:33:54Do No Harm Scores Major Victory Against Racial Discrimination in Medicine
Over the last several years, Do No Harm has repeatedly exposed the American Association of Family Physicians (AAFP) for its embrace of DEI and its forays into radical identity politics and activism.
The organization’s 2024 annual conference in September showed that the organization is as committed as ever to its ideological project. The conference was replete with references to DEI, radical policy proposals, and endorsements of gender medical interventions for minors.
Though the AAFP has long endorsed child sex change procedures, the way in which AAFP speakers discuss the issue is very revealing of the organization’s prioritization of agenda over evidence.
For instance, one presentation on so-called “gender-affirming” included claims that are flat-out false, and reveal an ideological commitment.
“There’s no question that it (pubertal suppression and cross-sex hormones) works; there’s no question that it saves lives,” said Molly McClain, MD, a professor of family and community medicine at the University of New Mexico. “The fact that it’s being questioned across this country and across the world is not about medicine and it’s not about evidence. It’s about politics.”
There is, in fact, more than a question as to the efficacy of child sex change interventions. The United Kingdom, Sweden, and Finland have all restricted these interventions. The Cass Review, an exhaustive examination of youth gender treatments within the United Kingdom, determined that the evidence for such procedures is of “poor quality.” Do No Harm recently released a report exposing the serious methodological flaws in the studies most often invoked to support so-called “gender-affirming care for children.”
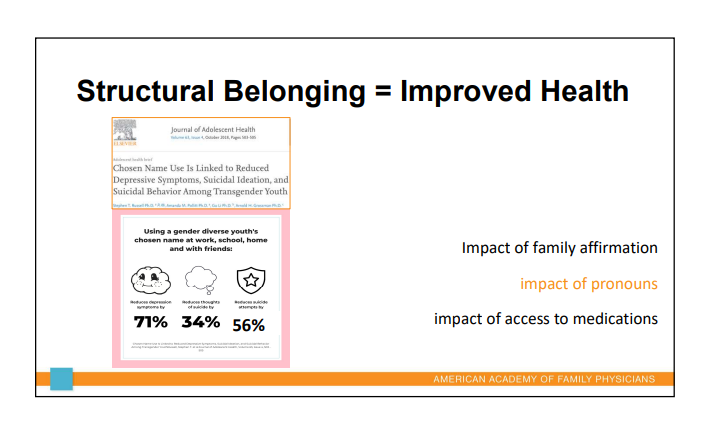
Figure 1. A slide on the impact of pronouns on mental health.
The presentation also called for “structural belonging” to improve outcomes among youth who believe they are transgender; in other words, a reorientation of society to “affirm” the chosen gender of the child. This includes pronoun use in basically every social setting.
In another particularly bizarre presentation, the face of President-elect Donald Trump was superimposed onto an anthropomorphic Cheeto to represent poor nutrition, with the caption “Cheeto-in-Chief.”
Figure 2. A slide featuring President-elect Donald Trump as a cheeto.
Other presentations included methods of achieving “lactation equity” that invariably involved policies such as “pay equity” and other political reforms.
But also, and more worryingly, the AAFP continued to platform misleading narratives surrounding implicit bias.
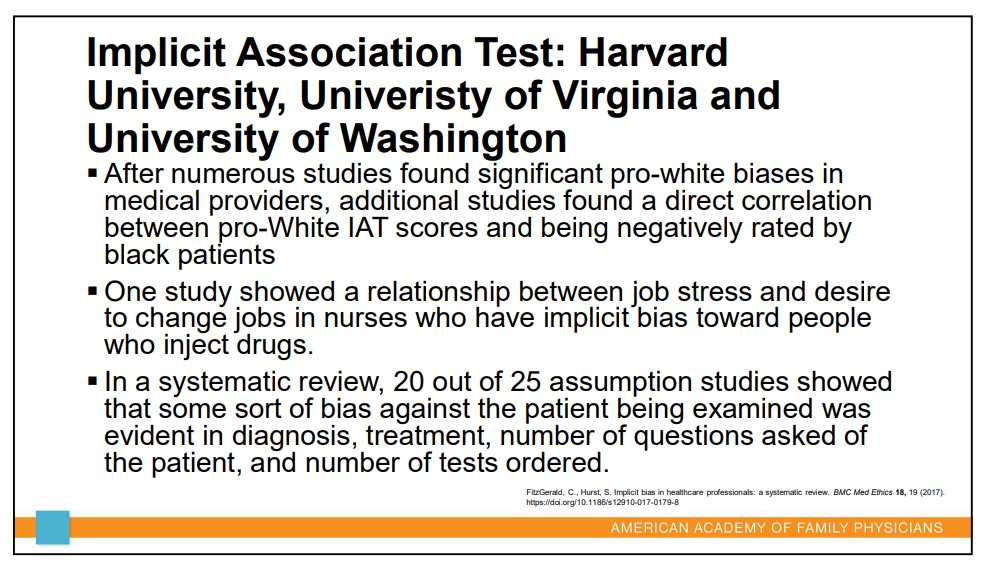
Figure 3. A slide discussing implicit bias.
Tests used to evaluate implicit bias fail to meet widely-accepted standards of reliability and validity; a 2013meta-analysis published in the Journal of Personality and Social Psychology found that the IATs were “poor predictors” of real-world bias and discrimination.
“Twenty years of research produced very little evidence that the IAT test predicts any real-world behaviour,” University of Toronto Mississauga psychology professor Ulrich Schimmack, who spent years studying implicit bias, said in 2019. “On top of that, some of the articles that claim it does, on close inspection, fail to show that.”
Nevertheless, the AAFP argues that implicit bias is a pervasive blight on healthcare leading to racial disparities in health outcomes. The presentation includes a video claiming that physicians are less likely to prescribe black patients pain medication, and implies this is due to physicians’ implicit bias.
However, the evidence for this claim is far from convincing. A systematic review of studies on racial disparities in pain medicine prescription published between 2011 and 2021 reviewed 15 cohorts and found that in only seven of them were black patients less likely to receive opioid pain medicine.
“Among 15 cohorts studied, 7 showed that Black patients were less likely to receive opioid analgesia, whereas 1 showed they were more likely to receive opioid analgesia compared to White patients,” the study found. “In the remaining 7 cohorts, there was no statistically significant difference in receipt of opioids between Black and White patients.”
Additionally, in several of the studies finding that black patients were less likely to receive opioid analgesia, the effect disappeared when controlling for socioeconomic status. This phenomenon indicates that socioeconomic status, rather than race, is the factor leading to this disparity.
But of course, that result is much less convenient to support the AAFP’s desired DEI agenda. After all, the AAFP’s Vice President of Medical Education explicitly endorsed racial discrimination in medical school admissions and decried the Supreme Court’s ruling against affirmative action.
The AAFP seems intent on staying the course and continuing its slide away from medical education and best practices and into political and cultural activism. Family physicians should ask themselves whether this organization is genuinely representative of their interests.
https://donoharmmedicine.org/wp-content/uploads/2023/12/shutterstock_1932378590-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2024-11-13 16:46:022026-02-11 15:33:54Family Physicians, Be Warned: The AAFP Doubles Down on Radical Ideology
In Season 3, Episode 9 of the Do No Harm Podcast, host Ian Kingsbury engages in a deep dive into the complex relationship between politics and medicine with special guest, Eric Kaufman, Ph.D, a distinguished political scientist. This episode examines the significant impact of political ideologies on medical practices and institutions, emphasizing the widespread influence of woke ideology and its downstream effects. As the nation reflects on a pivotal election, the conversation addresses the evolving political landscape and its consequences for DEI initiatives in healthcare. Tune in for an insightful discussion on preserving the integrity of medical practice amidst political challenges.
https://donoharmmedicine.org/wp-content/uploads/2024/11/Do-No-Harm-Podcast-S3-EP9-KAUFMANN-THUMBNAIL-scaled.jpg14402560rededge-rachelhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngrededge-rachel2024-11-12 21:33:062026-02-11 15:33:54S3E9: Exploring the Political Influence on Medicine
Nashville, TN; November 7, 2024: Today, Do No Harm, an association of medical professionals, filed a federal lawsuit to stop Tennessee’s unlawful consideration of race in appointments to state boards and commissions.
Tennessee medical practitioners fall under the purview of the Tennessee Board of Medical Examiners, while the state’s Board of Chiropractic Examiners oversees chiropractors.
A requirement of both boards, however, has nothing to do with medicine or chiropractic care, and everything to do with race. Three separate state laws force the governor to consider race when deciding who can serve on these boards.
“State medical boards are given important responsibilities to oversee the quality of care in their state and the safety of patients,” said Do No Harm Chairman Dr. Stanley Goldfarb. “It is crucial that they be the most qualified physicians available. Like all aspects of healthcare, patient safety and patient concerns should be primary, not the skin color or the racial makeup of any oversight committee.”
Tennessee is far from the only state that uses immutable characteristics to limit opportunities for individuals to serve their state and local communities. A report released by Pacific Legal Foundation,Public Service Denied, found that 25 states codify such unconstitutional discrimination. Pacific Legal Foundation is working to defeat race and sex quotas in Tennessee and everywhere else the unconstitutional practice is required.
“Tennessee law forces governor after governor to engage in racial discrimination when making appointments to state boards and commissions,” said Pacific Legal Foundation attorney Caleb Trotter. “Using race to make appointments to government boards is not only demeaning and unconstitutional, but it undermines the distinctive spirit of the Volunteer State by precluding opportunities for Tennesseans to serve their local communities.”
The case is Do No Harm v. William Lee and was filed in the U.S. District Court for the Middle District of Tennessee.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2024-11-08 17:07:592026-02-11 15:33:54Do No Harm Lawsuit Challenges Tennessee’s Racial Quotas for State Boards and Commissions
The NIH has long been one of the main vehicles for DEI to corrupt medical education and research. But after a Do No Harm fellow spoke out, in at least one instance that appears to be changing.
Back in February, the NIH announced a notice of intent to publish a funding opportunity for cardiovascular disease research through the National Heart, Lung, and Blood Institute (NHLBI). However, the notice made clear that the NIH prefers applicants to recruit certain racial groups for their study team.
“NHLBI expects applicants to recruit individuals from diverse backgrounds, including individuals from underrepresented groups for participation in the study team,” the notice said. For reference, the NIH’s diversity guidance defines underrepresented groups as “Blacks or African Americans, Hispanics or Latinos, American Indians or Alaska Natives, Native Hawaiians and other Pacific Islanders.”
The use of “expects” in the notice is key: the NIH wasn’t simply encouraging applicants to include these racial groups, but rather commanding them to do so.
If an applicant didn’t implement this bizarre racial preference, they wouldn’t get funding.
Do No Harm Senior Fellow Dr. Kevin Jon Williams, a professor of cardiovascular sciences at Temple University’s Lewis Katz School of Medicine, wrote a March op-ed in the Wall Street Journal highlighting the grant listing’s discriminatory guidelines.
Dr. Williams, who has African ancestry, could have noted his underrepresented background in his application for the grant and thereby increase his chances of getting funding.
Dr. Williams nobly elected not to do so, and chose not to validate the NIH’s discriminatory enterprise.
Now, following Dr. Williams’s op-ed, it seems the NIH may have gotten the hint.
In the actual funding opportunity listings posted in July for the cardiovascular research in question, the NIH dropped the language telling applicants they were “expected” to prioritize certain racial groups in their study team composition.
While applicants were still required to submit a Plan for Enhancing Diverse Perspectives (PEDP), the NIH said that the applications would be assessed based on “the scientific and technical merit of the proposed project,” and that “[c]onsistent with federal law, the race, ethnicity, or sex of a researcher, award participant, or trainee will not be considered during the application review process or when making funding decisions.”
This is quite a shift. The NIH went from instructing applicants to racially discriminate when constructing their study team, to now saying that it’s illegal to consider race at all!
The irony, of course, is the NIH was the one telling applicants to discriminate in the first place.
“The new administration in D.C. should be able to help the NIH return to its core mission,” Dr. Williams said. “The voting, tax-paying public does not want racial discrimination.”
As Do No Harm has extensivelycataloged, the NIH is one of the chief perpetrators of DEI in the medical field. And its diversity guidance still encourages racial preferences in prospective grant applicants.
But this is a step in the right direction all the same. The NIH should abandon its embrace of DEI and its support for racially discriminatory application criteria, and get back to what it should be doing: advancing humanity’s medical knowledge.
https://donoharmmedicine.org/wp-content/uploads/2024/07/shutterstock_1726134715-scaled.jpg14402560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2024-11-06 18:54:552026-02-11 15:33:54Is the NIH Softening Its Support for Racial Discrimination?