The National Institutes of Health is increasingly radicalized. We’ve already documentedhow NIH – the global leader in funding medical innovation – is elevating “racial equity” over research excellence. Now we’ve learned it’s embedding division and discrimination in the peer-review process.
Beginning in 2024, every peer reviewer for an NIH-funded study must complete so-called “implicit bias training” every three years. This training, as Do No Harm has shown, is grounded in the lie that some people are racist because of their skin color, while people of other skin colors are victims. There is no scientific basis for these generalizations, but then science isn’t the point. Implicit bias is a favorite tool of activists who want to reshape health care along racial lines.
Figure 1. Social media post regarding the mandatory training required by the NIH.
This mandate corrupts NIH research. Peer reviewers are supposed to do one thing and one thing only: Evaluate the accuracy of research projects. Instead, the NIH is encouraging them to look at research projects through a racial lens. Peer reviewers are less likely to have a critical eye for projects by minority researchers, while being more antagonistic toward projects from White and Asian researchers. Sure enough, NIH wants peer reviewers to “mitigate” their “potential biases,” which invariably means treating people differently based on skin color.
NIH has gained its prestigious reputation by fostering a highly competitive environment that elevates the brightest researchers and best projects. That’s why NIH funding has produced revolutionary advances, from gene therapy for hereditary diseases to immunotherapy for cancer. Now NIH is indoctrinating the peer reviewers who oversee research while accusing them of bias and racism.
The result will be less quality research and more racial division. The biggest losers will be the patients who need the NIH to continue funding medical breakthroughs, not radicalism.
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_1845309475-scaled.jpg14402560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-28 17:49:432026-02-11 15:33:40NIH Brings Racism Into Peer Review
Despite the U.S. Supreme Court’s ruling on June 29 that held race-based admission policies are unconstitutional in higher education, schools such as Ohio’s Wright State University Boonshoft School of Medicine (BSOM) have continued their race-focused planning and expensive DEI-related activities.
Freedom of Information Act (FOIA) documents obtained by Do No Harm show that Dr. Valerie Weber, dean of BSOM and a member of the administrative board of the Association of American Medical Colleges’ (AAMC) Council of Deans, sought data from the school’s director of admissions regarding the race and ethnicity of students offered admission in 2023 and 2024.
“We need this for the LCME [Liaison Committee on Medical Education] self study groups upcoming,” Weber informed Kaelin Locker, referring to America’s primary medical school accreditation organization.
An email dated July 18 reveals Weber asked Locker to complete a chart that provides “the total number of offers of admission to the medical school made to individuals in the school-identified diversity categories for the indicated academic years.”
The chart names “diversity categories” such as “Race/Ethnicity Classified as Under-represented in medicine (URM),” which is defined as:
African American/African/Black
Hispanic/Latin(x)
Native American/Indigenous Persons
Alaskan/Hawaiian/Pacific Islander
However, Dean Weber’s concerns regarding meeting presumed LCME requirements are unfounded, as Do No Harm reported on July 26. The previous day, the House Committee on Education and the Workforce heard the LCME’s explanation that its Accreditation Standards have nothing in them that “mandates which categories of diversity a medical school must use” to satisfy “focused recruitment and retention activities” or “mission-appropriate diversity outcomes.”
In other email documents obtained, it is clear the Supreme Court’s ruling banning race-based admissions is a concern to Weber.
On June 30, the day after the Court’s decision was released, Weber replied to a question posed by Amy Thompson, Ph.D., Wright State University’s provost and senior vice president of academic affairs:
You have obviously seen the Supreme Court decision regarding race based decisions. What is the plan to begin to suppress race and ethnicity on all Medical School applications?
“[A]ll applications are through AMCAS which is part of AAMC,” Weber responded. “They are analyzing the ruling and will be making changes accordingly. Essentially removing the identifier from the application is my understanding.”
In an email dated July 2, Weber shared AAMC’s statement that it is “deeply disappointed” by the decision, and then commented:
[M]edical school admissions is vastly different from undergraduate or graduate admissions, as we aim to select from a large pool those students who are best fit to pursue a career in medicine and fit BSOM’s particular mission. Medical schools follow holisitic [sic] admissions processes, and at BSOM, this involves looking at all aspects of our applicants beyond the numbers, strongly favoring Ohio residents and students from the region while aiming for a diverse student body. We also have accreditation standards around diversity which, I understand, will not be changing despite the decision. So, some challenges here as we move forward.
Nothing in the Court’s ruling says that schools can’t collect and analyze data or plan for future medical student cohorts. But just because race can no longer be considered in admissions decisions doesn’t mean it isn’t front and center in the minds of university administrators. Dean Weber’s emphasis on it shows that this information, as well as engaging in activities that align with the DEI agenda promoted by accrediting bodies, is still a primary focus – regardless of the costs.
The FOIA documents reveal that, on July 7, Weber engaged in another email discussion with Thompson. This time, the topic was related to an upcoming conference held by the AAMC.
In her email to Weber, Thompson appears to object to the cost of the conference after receiving requests for funding from Weber.
Thompson wrote:
The amounts requested are $4,000 and $3,700 respectively. There has already been considerable travel spend out of BSOM this last fiscal year and we need to set some reasonable parameters.
For these two trips, I will approve university spend of up to $2,200 for each of you. Any additional costs will have to be covered personally. Other colleges are not covering these high dollar expenditures for travel.
As a member of AAMC’s administrative board for the Council of Deans, Weber responded to Thompson’s resistance to the expenditures by justifying their significance, in part, because of her own role in the association.
Weber seemed to be pressing Thompson for additional staff to attend the conference for BSOM to get up to speed with “national norms”:
The meeting that you reference, the AAMC meeting, is not a meeting for faculty, it is a meeting attended by deans of medical schools and dean’s office staff. Because processes around accreditation are constantly changing, our engagement at the national level is needed. As you know, I sit on the administrative board for the Council of Deans. My attendance is needed and virtual attendance is not an option. My participation in this council is a very big win for BSOM and WSU as it gives us national visibility and input into decision making processes affecting all medical schools.
“When I came to BSOM, I heard that our dean’s staff had not attended this meeting in years, due to restrictions from the university, and I believe it is one reason why our processes have been so out of line with national norms, and why we are now working so hard to correct so much in time for the LCME,” Weber asserted. “Our Vice Dean, Dr. [Ngozi] Anachebe, came to us from Morehouse, having been a Student Affairs dean at their medical school for many years. She found it odd that she had never met anyone from our dean’s office. This was because they did not participate nationally in the AAMC, and had never attended this meeting.”
Weber added that while the cost of registration for the AAMC conference is high ($1,400), the meeting is not one “people are attending for their personal or professional advancement.”
“It is [a] mission critical to the school,” she stated.
These email communications illustrate that Wright State University’s leadership has been discussing its disappointment in the Supreme Court’s ruling and spending money on expensive conferences held by the same politicized organization that loudly expressed the same discontent. Do No Harm will be monitoring the actions of the Boonshoft School of Medicine and calls on its administration to apply merit to the medical school admissions process and focus on training competent doctors, rather than continuing to invest in identity politics. We encourage anyone with responsibility over the school’s administrative affairs to ensure that the leadership is committed to honoring the Court’s decision without reservation or equivocation.
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_2331689803-scaled.jpg19202560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-28 16:55:432026-02-11 15:33:40Wright State University Medical School Doubles Down on “Holistic Admissions” and Expensive AAMC Travel
A recent report of the Josiah Macy Jr. Foundation Conference on Ensuring Fairness in Medical Education Assessment promotes the idea that “Black and Hispanic” medical students who fail to successfully meet the demands of the rigors of learning assessments are victims of bias in the assessments themselves, and recommends “equitable” changes to assure more minority students are able to actually practice medicine.
The report, published in August at Academic Medicine, the flagship journal of the Association of American Medical Colleges (AAMC) – which assists in overseeing the Medical College Admission Test (MCAT) – says in its first sentence that “health equity” is dependent upon a “diversity” of races and ethnicities in the healthcare workforce.
“Health equity” is a narrative of diversity, equity, and inclusion (DEI) ideology, which, based in Critical Race Theory (CRT), claims “systemic racism” and “oppression” prevent minority individuals from obtaining access to sufficient health care. According to the radical dogma, if there are more minority physicians, more people from minority racial and ethnic groups will obtain higher quality health care.
The report of the Macy Foundation, which self-describes as “the only national foundation dedicated solely to improving the education of health professionals,” presents the problem of minority students who have been accepted into medical school with the use of DEI practices, but fail to make the necessary progress to advance through training to the actual practice of medicine:
Retention efforts so far have focused largely on addressing bias and discrimination broadly across the learning and working environment. A specific component of that environment—learner assessment—requires immediate, focused attention. Mounting evidence suggests that “bias plagues assessment” and can impede learners’ developmental progress and prevent some from advancing in the medical profession.
The report notes that one of the papers that became a “foundation” for the conference’s discussions on biased assessments was titled “The Long Shadow: A Historical Perspective on Racism in Medical Education,” a piece that described “the history of racism and oppression in American medicine” and explained “why understanding this history is crucial to advancing equity in medicine.”
According to the Macy report, the authors of the paper claim: “[W]e cannot meaningfully dismantle racial bias in medical education today without confronting its historic origins.”
The authors further described how “racism in contemporary medical education is a direct consequence of American medicine’s historical roots in European ideologies of White racial superiority, colonization, and slavery.”
The paper’s authors propose the following “actions” to confront racism in the field of medicine:
Incorporate the history of racism into medical education and unmask institutional histories of racism.
Create centralized reporting mechanisms and implement systematic reviews of educational and clinical activities for evidence of harmful bias.
Adopt “mastery-based” assessment in medical education.
Embrace holistic review and expand its possibilities in admissions.
Increase faculty diversity by using holistic review principles in hiring and promotions.
Leverage accreditation to combat harmful bias in medical education.
Another paper promoted in the Macy report addresses “harmful bias in the selection of medical residents.”
Proposed steps to ensure “historically marginalized” groups “will consider a certain specialty” include “thoughtful and strategic” outreach by residency programs to minority preclinical students, providing them with “specialized advising and sponsorship opportunities.”
Also recommended are “holistic applicant reviews,” ensuring interviewers are of various races and ethnicities who have been trained in “implicit bias reduction,” and “limiting interviewers’ access to normative learner assessment metrics, such as grades and exam scores.”
Despite numerous papers recommending modifications to guarantee more minority medical students can make it through to a residency program, the proposals applauded by the Macy Foundation all involve the potential of minimizing rigor while they attempt to ensure evaluators and interviewers are indoctrinated in CRT-inspired “implicit bias” ideology.
The foundation’s conference report suggests the following goals to achieve “fairness” in assessment:
Create a culture that promotes fairness in learner assessment
Design learner assessment systems that promote fairness and equity
Equip faculty and other assessors with the knowledge, skills, and funds to create learner assessment systems that eliminate harmful bias
Avoid overreliance on certain metrics; use holistic review for medical school admissions and residency selection
All members of the medical education community must commit to and work toward achieving fairness and equity in learner assessment
While the Macy Foundation promotes diversity as a primary goal, a new study focused on the performance of emergency medicine residents raises concerns about the “danger” associated with “elevating diversity over quality in medicine.”
Do No Harm Chairman Stanley Goldfarb, M.D. cited the study in October at National Review, noting that its woke authors observed that all residents who participated in the research were found, by faculty, to have performed equally at the start of their training, but that, over the next three or four years, minority residents, especially women, were judged to have demonstrated less competent patient care.
“Naturally, the researchers conclude that so-called ‘intersectionality’ is to blame,” Goldfarb wrote, but challenged that conclusion with the common sense explanation that “the fact that all the residents were judged to perform equally at the initiation of their training is not surprising and is quite typical, indicating that the faculty is not suffering from bias.”
“The authors would have us believe that bias develops over trainees’ time in the program,” Goldfarb continued. “Yet it’s far more likely that, with time and experience, the faculty recognize which trainees are performing well — and which aren’t.”
An “unfortunate yet increasingly common reality,” he also pointed out, is that prior poor performance in medical school “is simply continuing into residency.”
And that, Goldfarb asserted, is what happens when “standards have been lowered in the name of diversity.”
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_1994910104-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-27 23:54:542026-02-11 15:33:40Macy Foundation Promotes DEI Dogma that Minority Medical Students Fail Due to Biased Medical Education Assessments
On November 10, 2023, Do No Harm Chairman Dr. Stanley Goldfarb spoke on The Impact of DEI Policies on Medical Education and Healthcare at the Bagwell Center at Kennesaw State University’s Coles College of Business. A link to the Bagwell Center’s podcast episode featuring Dr. Goldfarb’s speech is available here. Below are the remarks as prepared for delivery.
Good afternoon.
I’d like to thank the Bagwell Center for this kind invitation and the opportunity to speak with you about the crisis that’s unfolding in American medicine and, in fact, in American life in general.
My interest in the impact of the so-called Diversity, Equity, and Inclusion regimens (or DEI) began about eight years ago when I realized that my medical school, the Perelman School of Medicine at the University of Pennsylvania, had embarked on a new direction driven by new senior leadership in the School of Medicine. I was serving as the associate dean for curriculum at that time. The new plan was aimed at drastically altering the medical education program at Penn.
What had been a traditional approach focused on clinical science and aimed at developing medical leaders was being readied for transformation into a far greater emphasis on community involvement and concern for social issues. The rationale for this was the hypothesis that the root cause of disparate healthcare outcomes between minority, particularly black, and majority communities was the result of bias on the part of physicians and healthcare institutions, and only through a dramatic reimagining of the practice of medicine could these disparities be eliminated.
Now, unlike many fields where the academic training is divorced from the world of practice and has little influence on the community of practitioners, medicine is quite different. The goings on in law schools have traditionally had little to do with the actual practice of law and have had minimal influence on the practice of law. The same is true in many fields of endeavor. But medicine is quite different in that the academic health center is the driving force in local healthcare and has great influence across the nation. American academic medical centers have been the engines of advances in the treatment and cure of diseases. What happens in academic medical centers doesn’t stay there but diffuses out into the community in general.
As it turns out, the expanding focus on social issues in medical care was well established in other medical schools and our school was rather late to the game. We did have courses that discussed some aspects of the West Philadelphia community, a very heterogeneous community with large and varied immigrant populations, but this was felt to be insufficient. The new vice dean of the medical school told me that there was “too much science in the curriculum.”
My concerns about the new initiative to modify Penn’s curriculum and my growing awareness of the fact that medical schools around the country were much further along in adopting an approach that seemed to echo the curricula of schools of social work led me to speak out on this issue. I felt that medical school curricula should maintain a strong focus on medical science, should increase its rigor, and should concern itself with turning out the highest quality physicians who would care for those suffering from illness. I also felt that while social factors are important in defining the quality of life in communities, physicians had no agency in influencing such issues as poor housing or community violence. It seemed that the purpose of training physicians in these issues was to create advocates for political solutions to these problems rather than training physicians to improve healthcare outcomes.
In 2019, I wrote an op-ed in the Wall Street Journal about my sense that medical education was heading down a path that would weaken American healthcare. The Wall Street Journal decided to entitle that article “Take Two Aspirin and Call Me by My Pronouns.” This elicited a rather strong reaction on Med Twitter and really began my new career as an activist.
This background explains why I am here today speaking with you about this issue. Four years have now passed and increasingly, the impact of DEI programs that focus on identity politics in the recruitment of medical practitioners and in the manner patients are to be treated has become more and more evident. Recently, Wesley Yang, one of the editors of Esquire magazine posted my article from 2019 on Twitter and commented, “Shouldn’t we have listened to him then?” It is tough being Cassandra, the mythic Greek figure who could predict the future but no one would listen.
So what is happening to American healthcare in the DEI era? The pandemic and the death of George Floyd clearly marked a turning point in this saga. We began to see the impact of identity politics, a phrase that I feel describes the underlying principles of DEI. Yascha Mounk has written a new book entitled The Identity Trap. He, a self-described liberal and a professor of political science at Johns Hopkins, decries the impact of identity politics on American life. I quote from his book, “The identity trap poses serious dangers. It undermines important values like free speech. Its misguided applications have proven deeply counterproductive in areas from education to medicine. If implemented at scale it won’t provide the foundation for a fair and tolerant society; it will inspire a zero-sum competition between mutually hostile identity groups.”
His concern, which I share, is that this political and philosophical theory, known as Critical Race Theory (CRT), paints a hostile and irredeemable society based on oppressors and oppressed, and will lead to division and conflict. It will poison the American experience.
I think we can discuss this issue from two perspectives: the impact of identity politics on the practice of medicine and the impact of identity politics on who can practice medicine.
Dr. Stanley Goldfarb, Do No Harm chairman, addresses students and guests at Kennesaw State University on November 10, 2023.
Healthcare disparities between minority and majority populations are real and of legitimate concern. But attributing them in large part to the black community’s oppression by white males and the healthcare system in general is without real proof and without merit. As Mounk points out in his book, once group identity is viewed in the formulation of either being oppressed or an oppressor, a fixed set of responses ensues. Oppression is unending and can only be overcome through conscious and illiberal actions. Accepting this formulation requires, in the words of Ibram Kendi, a discriminatory regimen. To quote him, “past discrimination can only be remedied by present discrimination, present discrimination can only be remedied by future discrimination.”
During the COVID pandemic we received a taste of how this all could play out. When monoclonal antibodies were a potential lifesaving treatment for severe cases, two states, California and New York, created guideline algorithms that gave points toward justification for the use of the drugs in particular cases based on race. The use of the scarce drugs would be determined in part based on skin color rather than purely on medical need. This violates the Hippocratic Oath but is in concordance with Critical Race Theory.
In a second instance, the Centers for Disease Control, the CDC, recommended to states to give essential workers access to the mRNA vaccine even ahead of the elderly on the grounds that older Americans are disproportionately white. Amazingly, some of the most prominent medical institutions such as the American Public Health Association (APHA), the American College of Physicians (ACP), and the American Medical Association (AMA) supported this approach with amicus briefs when it was challenged in the courts.
These two examples show how simply enacting the principles of Critical Race Theory can have a profound impact on the lives of individual Americans. But at least in these cases, there was no attempt to hide the rationale behind the actions. There was complete acceptance of racialism. What’s more concerning, has been the misuse of medical studies to justify unequal treatment on the grounds that it will improve healthcare for minority groups.
Let me describe two examples. Two prominent physicians at a major Harvard teaching hospital published a study in the Journal of the American College of Cardiology (JACC) claiming that there had been discriminatory practices in the emergency room in the treatment of patients who entered with a diagnosis of congestive heart failure. Approximately 57% of white patients who entered with that diagnosis were referred to a cardiology specialty service in the hospital for cardiac care. Approximately 45% of black patients with the same diagnosis were referred to the specialty unit. The alternative unit for admission was a General Medical unit. This discrepancy was presented as proof of racism and led them to propose a new paradigm for care. Black patients would be asked which unit in the hospital they wished to be admitted to.
As it turns out, and as is often the case when comparing two populations of patients, the individual characteristics of the patients govern treatment protocols rather than their skin color. In this instance, the black patients suffered disproportionately from chronic kidney disease and were being treated with renal replacement therapy using hemodialysis. Such patients are better treated on the General Medical unit where hemodialysis treatments are effective in controlling heart failure and are more easily arranged. White patients disproportionately had their heart failure on the basis of intrinsic cardiac disease which required special procedures only available in the cardiac unit.
The researchers ignored the role of these patient characteristics in the admission decision and instead blamed it on physician bias. They so accepted the oppressor/oppressed binary of Critical Race Theory that critical thinking was out of the question.
Rather than focusing on the individual patient characteristics, their new paradigm was to focus on skin color, even though this could possibly lead to worse care because of admission to the wrong unit in the hospital. Ultimately, this approach was not enacted but currently the electronic medical record prompts any admitting physician to consider the past discriminatory practices which were, in fact, not discriminatory.
A second example comes in the recent enthusiasm for the concept of patient-physician racial concordance. Multiple organizations such as the Association of American Medical Colleges (AAMC), the trade organization of American medical schools, have written that those disparities that black patients experience in health outcomes can only be remedied by having a black physician. They typically cite one or two studies that they claim show such a benefit, again misinforming other practitioners and the public.
Careful study of the medical literature of this issue reveals a very different picture. Our organization, Do No Harm, about which I will speak shortly, has examined this issue in a comprehensive study by our Director of Research Ian Kingsbury and Jay Green of the Heritage Foundation. They have found that there is no valid study to support the claim that health outcomes improve if black patients have black physicians. Those organizations that claim this to be true are simply ignoring facts in favor of an unproven theory.
Critical Race Theory will do that to you; it will demand ignoring facts to support the oppressor-oppressed dyad. For example, there are 42 studies of whether black patients and black doctors communicate better than when the dyad consists of a white physician and a black patient. Six studies do show more satisfaction with communication by black patients. However, eight studies show worse communication when black patients had a black doctor. Twenty-six studies showed no difference when the physician was white or black and the patient was black. Yet, DEI bureaucrats claim that more black physicians are required in order to improve health outcomes. The divisiveness that Yasha Mounk described in his book The Identity Trap is on display here. Do we really want black patients coming to clinics and demanding black doctors? Do we want white patients entering healthcare institutions and demanding that they only see white physicians? I witnessed bigoted patients making such demands during my days as a clinician. When patients made such demands at our hospital, we told them to seek another hospital.
Another consequence of this model is the conclusion that black patients don’t seek the best medical care and are more interested in the race of their healthcare providers. How demeaning to black patients!
This concept of racial essentialism as a guiding force in American life will only lead to more conflict because individual characteristics become sacrificed for group identity. Mounk calls this idea an identity trap; a trap, because it seems attractive on the surface but once entered becomes difficult if not impossible to escape.
There are many other examples of how the medical literature is being distorted in the service of Critical Race Theory and its demands that so-called “anti-racism” be practiced in order to improve healthcare outcomes. In reality, the solution to healthcare disparities is not ineffective or counterproductive implicit bias training for physicians but rather it is better health access for patients. Minority communities do not need different healthcare, they need more healthcare.
Dr. Stanley Goldfarb at Kennesaw State University on November 10, 2023.
The second area where Critical Race Theory and its implementation through DEI and identity politics will have a profound influence on healthcare is through the admission process into medical school and the promotion process for faculty. We have been told the rationale for seeking a medical school class whose components perfectly reflect the racial distribution of America is better healthcare outcomes. We have been told by the AMA, by the American College of Physicians, and by the Association of American Medical Colleges that diversity improves healthcare outcomes. They say this but they have no data to support this idea. In many areas of American life, diversity may be a perfectly appropriate basis for recruitment and hiring. But what about pilot school? What about neurosurgery?
In most debates about school admissions, the discussion centers about the interests of the school and the interests of the student. In certain critical professions however, a third entity must be part of the discussion. In healthcare it is the patient. When considering entry into medical school, the individual patient’s interest must be a primary concern. Unfortunately, identity politics declares that the students’ race must be an important determinant. While it is true that the recent Supreme Court decision in the case of Students for Fair Admissions v. Harvard seems to have eliminated so-called affirmative action as a basis for admission to university, many medical schools have announced their intention to ignore this principle and to produce workarounds to allow continued efforts to increase racial diversity.
Part of the justification for this particular brand of affirmative action is that if students can pass minimal competency exams, like licensure exams, then they are qualified to be physicians. Therefore, seeking out the best and the brightest who have been particularly successful in their academic pursuits is really not necessary to produce adequate healthcare. But this is not what patients expect. No matter what their racial background, patients expect and should receive the highest possible quality of care.
Academic achievement by physicians is an ingredient in creating a highly effective physician workforce. I have maintained that medicine is a highly academic pursuit. I point out to students that the way we test their knowledge is through multiple choice questions on exams. In this model, there is a stem, a short statement about a particular patient or a particular medical condition, and then a series of five distractors or possible explanations as to the origin of the clinical problem. Their job is to pick out the right answer. And I tell them that when they enter the clinics and begin to see patients, they will be constructing the multiple-choice question. They will gather the information required for the stem or description of the problem. They will then produce four or five alternative possibilities to explain the problem and pick the right one to properly care for the patient.
This is an academic process. This requires maintaining much information about illness and about the variability of human response to it and it requires judgment that is abetted by a strong understanding of the basic principles underlying the clinical problems that they encounter. This activity requires a nimble mind and the commitment to learn a vast amount of information to deal with patient problems in real time while in the presence of the patient. There is no time to retire to the library to learn about the patient’s problem.
How has the healthcare system and academic medicine responded to this challenge? They have decided that it is more important to pick students based on racial characteristics and it is more important to have a racially diverse corps caring for patients in various medical specialties than it is for identifying the most capable individuals to take on those roles. To achieve this diverse system, there has been a growing movement to eliminate traditional academic qualifications for entry into medical school and for selection to the most competitive postgraduate training programs. The MCAT, the achievement test for medical school entry now includes more social science and less hard science. The Council of Deans of medical schools has now decreed that grades will no longer be reported for the licensure exam that has been used as an achievement test to determine merit and likelihood for success in some of the most challenging medical specialties. This minimal competency exam is now pass/fail. They expressly state that the reason for this rule is to increase the numbers of minority applicants who succeed in gaining places in the most competitive training programs.
This downgrading of academic performance and reliance on so-called holistic measures to determine admission to medical school is already leading to evidence of decreased performance in the clinical arena. There are now two large studies that show that minority residents perform less well. In a survey of three institutions’ internal medicine residency program and in a nationwide study of emergency medicine trainees, minority trainees as a group perform less well in multiple assessment domains including professionalism, medical knowledge, and preparation for practice. This is not to say that there aren’t very high performing, high quality minority individuals who were entering these fields. But rather it says that the training programs and medical schools, in some instances, have sacrificed merit in the name of identity politics. There are 22,000 medical students entering medical school each year. There are almost 44,000 applicants for a position in medical school each year. This is a zero-sum game. If a qualified applicant is not admitted in favor of an unqualified or lesser qualified one, that qualified individual may never have the opportunity to become a physician. It is not like undergraduate years where individuals have a multitude of options for their education.
The drive for diversity in medical school classes has led to a concomitant decline in the rigor of medical education. I believe these two issues are linked and mutually supporting. Fifty years ago, the attrition rate of medical students averaged nine percent nationally although it was as high as 14 percent in some schools. Today, the attrition rate in medical education is less than three percent. This reflects an unwillingness to remove all but the most egregious examples of academic failure from medical school classes.
Grading in the preclinical years of medical school is now almost universally pass/fail. At Harvard, in a recent graduating class, 92 percent of the students received an honors grade for their clinical work. When this occurs, there is essentially no such thing as “honors” and no real grades. The fault for this set of circumstances lies with both the faculty and the students. Faculty feel compelled to guarantee that students can pass the curriculum and graduate. Faculty performance is graded by students who tend to downgrade faculty members who demand extreme rigor in classwork.
So too has the recruitment and promotion of faculty been diminished by DEI. Many medical schools now actively declare that they specifically seek to hire black faculty. If they can identify highly qualified faculty that happen to be black, that is one thing. But if they choose faculty on the basis of race, that is no different than denying an opportunity on the basis of race.
The DEI regimen also demands that faculty seeking promotion be able to demonstrate not only that they support Diversity, Equity, and Inclusion but that they have actively worked to promote this divisive idea. This is an example of compelled speech at institutions that purportedly honor freedom of speech principles.
The idea that research faculty should also adhere to DEI principles and that the recruitment of such faculty should be closely overseen by representatives of the DEI offices of medical schools is particularly absurd. The privilege of performing research, particularly laboratory research, is reserved for those with both the drive and the intellectual capacity to be creative and to make important contributions to the health of the American people. There is no rationale for injecting a diversity requirement in recruiting individuals or promoting individuals who are scientists. The NIH has recently downgraded the role of faculty expertise or institutional resources in determining who will receive the highly competitive individual research grants. Sacrificing merit on the altar of diversity can only lead to a less meritorious scientific enterprise.
Lastly, I would like to slightly divert this discussion to confront the most recent manifestations of DEI in the outpouring of anti-Semitic vitriol in America. The healthcare system, unfortunately, is well represented in those tearing down posters of kidnapped children and those equating the slaughter and rape of women, children, and the elderly by Hamas terrorists with Israel’s legitimate efforts at eliminating a barbarous enemy.
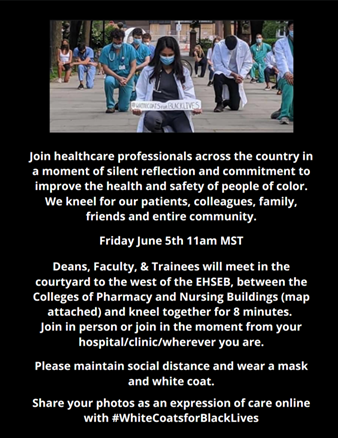
Medical organizations like White Coats for Black Lives have expressed support for the atrocities that Hamas is so eager to publicize.
There is a clear nexus between identity politics, Diversity, Equity, and Inclusion programs, and anti-Semitism. In each case, traditional Judeo-Christian ideas about morality have been replaced by the tenets of Critical Race Theory.
Simply judging Israel as the oppressor eliminates all responsibility for even the most barbarous actions by the “oppressed” Palestinians. In this way, the vile declarations by physicians on social media who praise Hamas terrorism are substituting Critical Race Theory for traditional morality and reliance on facts to make moral judgments. Thus, the actual independence of Gaza after Israeli withdrawal in 2005 is called “occupation.” The movement of over 17,000 Gaza residents each day into Israel for employment on October 6 is called an “open air prison.” The killing of young women, children, and the elderly is justified as they are part of the oppressor class. The values passed down to western civilization through the Decalogue are now replaced by Critical Race Theory as our moral compass.
I would like to conclude this rather morose view of the effect of DEI on the world of medicine by highlighting some hopeful signs. In April 2022 we founded Do No Harm, a non-profit organization devoted to combatting Critical Race Theory’s corruption of healthcare. It is a membership organization and now numbers over 6,000 healthcare workers and concerned patients as its members and has members in 14 countries.
We have worked to inform the public about this danger through over 4,900 mentions in print and online media, 25 op-eds and editorials in the Wall Street Journal, the Washington Post, and other top outlets, and over 50 appearances on television. We have strived to contain the DEI regimen through legal and legislative efforts around the nation. We have initiated five lawsuits against defendants like the Medicare System, Pfizer, the Journal of Health Affairs, the Arkansas State Medical Board, and the state of California. In conjunction with our senior fellow, Mark Perry, we have initiated hundreds of letters with the Office for Civil Rights in the Department of Education protesting discriminatory fellowships and scholarships at a variety of public institutions. And finally, we have worked with leading national law firms to generate model legislation to combat DEI activities in a variety of public institutions that depend on state support.
Over and over again, we have found support in physicians and students in many medical schools and academic medical centers. They understand the danger that DEI poses to the American healthcare system. They object to the divisiveness and the discriminatory practices that the DEI regime promotes.
Some important commentators have begun to express hope that the “woke mind virus,” in the terminology of Elon Musk, is beginning to face serious questioning. The recent American descent into anti-Semitism has been directly tied to the identity politics at the heart of DEI. When we stop seeing people as individuals and relegate them to group identity, bigotry and hate are the next stage of social evolution. The public is starting to notice this consequence, and that spells hope for the re-emergence of the American idea of individual value and individual responsibility.
Are you interested in inviting a Do No Harm expert to speak to your group? Let us know by requesting a speaker here.
https://donoharmmedicine.org/wp-content/uploads/2023/11/Kennesaw-speech-announcement.jpg306548supporthttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngsupport2023-11-24 10:30:002026-02-11 15:33:40Dr. Stanley Goldfarb Speaks on DEI in Medicine at Kennesaw State University
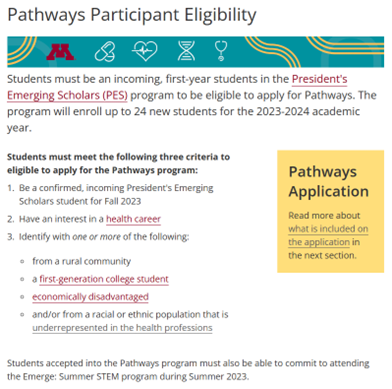
The University of Minnesota (UMN) has changed the eligibility criteria for a pre-health student scholars program that was illegally discriminating on the basis of race. Title VI of the Civil Rights Act of 1964 prohibits such discrimination, and the Health Profession Pathways initiative at UMN was excluding certain students based on their race, color, or national origin.
In the complaint filed with the Department of Education’s Office for Civil Rights (OCR) on May 27, 2023, Do No Harm program manager Laura Morgan provided evidence of racial discrimination in the eligibility criteria of the Pathways program. According to the program’s website (archived page), students must “Identify with one or more of the following, which included“and/or from a racial or ethnic population that is underrepresented in the health professions.”
Figure 1. Archived page for the Health Profession Pathways program at the University of Minnesota (May 27, 2023).
The federal civil rights investigation was opened on November 2, then was closed on November 17 after UMN “provided OCR with information that it has revised the eligibility criteria for the Program to remove any racial criteria or preference.” On the current website, the third bullet point has been removed, and UMN informed OCR that, “during the time relevant to this complaint, the University received applications from and offered admission to the Program to students who are not Black, Mexican Americans, Native American or mainland Puerto Rican.”
Figure 2. Revised eligibility criteria for the Pathways program at UMN (November 17, 2023).
“The University of Minnesota has the notoriety as being one of the worst serial offenders of federal civil rights laws in the country,” said Do No Harm senior fellow Mark Perry. “UMN has been the target of more than 25 separate complaints over the past five years for more than 50 violations of Title VI and Title IX.”
“While Do No Harm is pleased that at least one of those civil rights complaints of race-based discrimination has been successfully resolved in our favor,” Perry continued, “we are calling on Minnesota’s premier taxpayer-supported public institution to correct its dozens of other ongoing violations of federal civil rights laws.”
More institutions of higher education must remove scholarships and programs that discriminate against applicants based on race or sex. Do No Harm will continue to take action against these initiatives to compel colleges and universities to comply with federal civil rights laws and provide equal opportunity to all qualified individuals.
If your school is violating Title VI or Title IX by discriminating on the basis of race or sex, please let us know.
https://donoharmmedicine.org/wp-content/uploads/2022/12/shutterstock_2038801634-scaled.jpg17062560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-22 23:05:002026-02-11 15:33:40The University of Minnesota Quickly Cleans Up a Discriminatory Pre-Health Program In Response to a Federal Civil Rights Investigation
How do “diversity, equity, and inclusion” policies and practices find their way into unexpected places outside of major city centers and deep blue states?
A major hospital system in Georgia’s northeastern corner, one of the reddest parts of the state, provides an answer.
Northeast Georgia Health System (NGHS) serves about 1 million residents in 19 counties. NGHS is a five-campus, not-for-profit 850-bed community health system that countsitself among the 20 largest employers in the Atlanta region. Its more than 9,000 employees include a medical staff of about 1,500 representing 60 specialties.
Although the NGHS nondiscrimination statement claimsit “complies with applicable Federal civil rights laws and does not discriminate” and “does not exclude people or treat them differently because of race, religion, color, national origin, age, disability or sex,” a closer look finds much to question.
The reality is that NGHS pushes radical diversity, equity and inclusion (DEI) practices – the kind of practices that reinforce discrimination and disparate treatment, both in healthcare and in the workplace.
One such offering is the DEI scholarship offered by the Emergency Medicine Residency DEI committee for visiting medical students. Applicants must be from a “historically underrepresented group;” however, the eligibility criteria exclude whites, as well as Asians who are not “Filipino, Hmong, or Vietnamese.” Applicants must also explain, “What does diversity, equity and inclusion mean to you?”
Figure 1. Application for the Emergency Medicine DEI Scholarship at the Northeast Georgia Health System.
Here are some additional examples of how NGHS embeds DEI into every corner of its operations:
NGHS’s Continuing Medical Education (CME) program has hosted lectures and DEI training since at least 2020, where physicians and nurses earned continuing education credits. Speakers included the “founder of antiracism,” Ibram X. Kendi, in April 2021. Kendi is famous for teachingthat “The only remedy to past discrimination is present discrimination; the only remedy to present discrimination is future discrimination.” In his Zoom webinar, titled “Teach Antiracist Practices,” Kendi told his NGHS audience, “Most people hold racist beliefs and ideas.”
NGHS’s Graduate Medical Education DEI program’s mission is “to acknowledge institutional and systematic biases with the goal of supporting resident physicians and fellows on socioeconomic, gender and ethnicity-related healthcare disparities … to promote healthcare equity.” The program has a “Medical Staff Diversity & Healthcare Disparity Taskforce,” which addresses “issues surrounding diversity” within the medical staff. The Taskforce also places an emphasis on “community healthcare disparities,” but does not define them.
Virtual reality DEI simulations from the Center for Simulation and Innovation (CSI) “immerse and train resident physicians on current healthcare disparities.” A 2021 technology grant awarded for DEI virtual reality simulations included another goal: “to incorporate specific diversity, equity, and inclusion training into resident curriculum.” The CSI team’s presentationsat an international conference in January included “How to Design/Implement Your Own DEI Virtual Reality Platform.”
A 2022 DEI grantfrom the NGHS Foundation funded a project to investigate how FitBits affected health behaviors of “socially disadvantaged COVID-19 survivors.”
Other NGHS lectures covered the effects of “unconscious bias” on healthcare decisions and results, along with “Mobilizing for Healthcare Equity.”
Figure 2. Educational offering from the Northeast Georgia Medial Center Department of Emergency Medicine.Figure 3. Educational offering in the “Diversity in Medicine Lecture Series” at NGMC.
Such prioritizing of DEI should come as a huge surprise to patients of NGHS, who want great care irrespective of skin color or background. As for staff, they have alerted us that they take offense at the presumption that biases, affect their treatment – and therefore the health outcomes – of those who walk in the doors of Northeast Georgia Health System.
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_2013565328-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-21 13:39:102026-02-11 15:33:39Hospital System Injects Woke DEI Practices Into Northeast Georgia
The University of Tennessee (UT) and the University of Utah (UU) are refusing to release email communications between key school leaders regarding the recent conflict between Israel and Gaza. Both schools have a history of hosting and even kowtowing to demands from an extremist student group that directly aligns itself against Israel.
Do No Harm submitted a Freedom of Information Act (FOIA) request to a number of schools following incidents of anti-Semitic hate and perpetuation of radical ideologies by White Coats for Black Lives (WC4BLUMN). Spawned by Black Lives Matter, WC4BL has a presence in several schools of medicine across the country. Following the attack on Israel on October 7, the national organization for WC4BL released a statementfalsely claiming that Israel was committing “genocide” and showing clear support for “Palestine’s struggle for liberation.”
Figure 1. Do No Harm post on X regarding White Coats for Black Lives (October 20, 2023).
We asked for email communications from specific administrative personnel, such as university presidents, chancellors, provosts, medical education deans, student affairs personnel, and leaders in DEI departments. Keywords we submitted in our FOIA request are:
Hamas
Gaza
Israel
Palestine
Palestinian
Middle East
Ukraine
Jew
Jewish
Arab
Islam
Muslim
Antisemitism
Islamophobia
Tennessee and Utah’s responses to our FOIA requests for communications about the situation suggest that there’s something in the emails that UT and UU don’t want the public to see.
Citing state law (Tenn. Code Ann. § 10-7-503) from the Tennessee Public Records Act) in its denial, the University of Tennessee says that our FOIA request is “overly broad and not sufficiently detailed,” adding that it would require the school to “sort through files and search through voluminous records” to fulfill the request. The response concludes by stating that Do No Harm’s request “constitutes an improper attempt to use the Public Records Act as if it were a discovery request made pursuant to litigation.”
A follow-up request is pending. But in the meantime, it’s notable that the University of Tennessee System has engaged in WC4BL events in the past, and the UT Health Science Center has a webpage dedicated to the group.
Figure 2. WC4BL demonstration at the University of Tennessee (Fall 2020).
A similar reply was received from the University of Utah, which justifies the withholding of public records by referring to its Government Records Access and Management Act (GRAMA, section 63G). Specifically, the school responded by saying:
Your request does not identify the records sought with reasonable specificity, as required by GRAMA. Id. § 63G-2-204(1)(a)(ii). In addition, the University may consider whether it is able to fulfill certain requests without unreasonably interfering with its duties and responsibilities. Id. § 63G-2-201(9). The University cannot respond to your request without more specific information concerning the particular records you seek. Therefore, we are unable to respond your request as initially presented.
We have contacted UU’s general counsel for further explanation and are awaiting an answer. However, the school also has a history of WC4BL support.
The Campus Connect platform at the University of Utah confirms that WC4BL is a sponsored student organization at the school. During the summer of 2020, the University of Utah Medicine chapter of White Coats for Black Lives “peacefully presented a list of demands” to the dean and vice dean of the school. The demands included cutting ties with local police and creation of a plan to “matriculate a first-year class in 2021 with overrepresentation of Black, Latinx, Native American and Pacific Islander/Native Hawaiian students.” The Anti-Racism Commission (archived page here) was subsequently formed by a group of students from WC4BL, producing a full report. And, in late 2021, medical students and personnel joined UU’s deans and faculty for a demonstration coordinated by WC4BL.
Figure 3. WC4BL demonstration at the University of Utah (December 28, 2021).
Current events on American college campuses illustrate how “toxic DEI ideology” leads to radical assertions by student groups like White Coats for Black Lives with an agenda to push. Campus leaders undoubtedly have something to say about it. Why are the University of Tennessee and the University of Utah hiding what their chancellors, deans, and DEI leaders are discussing?
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_1712900470-scaled.jpg17062560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-20 12:57:002026-02-11 15:33:39Two Major Universities Deny Requests for Communications About the Hamas Attack on Israel
On October 7th, Hamas butchered more than 1,200 men, women, and children in southern Israel. Within days, the medical student association “White Coats for Black Lives” (WC4BL) accused Israel of committing “genocide.” The Minnesota chapter clarified that Palestinians should “free themselves from their oppressors by any means necessary.”
Neither the national organization nor Minnesota chapter faced any professional sanction. Ostensibly emboldened by the lack of consequences for espousing blood libel and calls to genocide, the national organization released a new statementon November 8th complaining that some medical professionals who voiced similarly despicable ideas did in fact suffer consequences.
An increasing number of American medical institutions have moved beyond their complicity with the U.S.-funded genocide of Palestinians, either through their silence or Zionist statements, to personally target Palestinian and Palestinian-American healthcare providers advocating for the freedom of their own people, and their allies. This is a violation of the human right to resist the mass murder and dispossession of one’s own people, and allies’ rights to stand in solidarity. In addition, medical institutions’ participation in Zionist doxing further fuels Islamophobia and endorses anti-Palestinian and anti-Arab discrimination. For the reasons described above, we demand:
All American medical institutions immediately reinstate all healthcare providers who have been fired or placed on leave for demanding a ceasefire, the end of the siege on occupied Gaza, and the end of Israeli occupation, or have affirmed Palestinians’ right to resist in the face of 75 years of relentless oppression.
Involved institutions issue public apologies to impacted healthcare providers.
All disciplinary actions are removed from the records of impacted providers.
Offending institutions offer any needed letters explaining disruptions in training or work which explicitly state that the disruption was the result of the inappropriate actions of the institution.
Institutions retract all statements denouncing healthcare providers in solidarity with Palestine and any associated punishments.
Institutions immediately end efforts to intimidate pro-Palestine medical workers into silence (e.g. through disciplinary or professionalism meetings, threatening emails, encouraging a culture of reporting those in solidarity with Palestine, etc.).
The letter goes on to name four individuals that WC4BL believes worthy of reinstatement and deserving of public apology from their employers. Just who are these martyrs?
Tania Singh claims to have been fired from a nursing job for—as she frames it in a gofundme page—taking a stance “that’s way too unacceptable for a settler colonial nation.” She offers more detail in an interview with The Masses, the self-described “official press organ of the Revolutionary Maoist Coalition.”
Singh: I wrote something like “it will be a cold day in hell when the colonizers get to lecture the colonized on how to resist”…I was terminated on the following Friday for antisemitism, support of terrorism, and harassment.
Interviewer: It’s telling that as soon as support for Hamas comes up that’s a red line.
Singh: Exactly! And if it wasn’t Hamas it would be someone else.
Singh was given a platform to share her story and used the opportunity to lean into the microphone and repeat her support for terrorism. WC4BL apparently nonetheless believes that Singh is owed an apology and not owing of one.
Dana Diab was an emergency room physician at Lenox Hill Hospital who shared a video of the massacre that occurred at a musical festival near the Gaza border with a caption that read “Zionists colonists get a taste of their own medicine.” She was fired, but she would still be practicing medicine if WC4BL had their druthers.
Zaki Massoudtook to Instagram after the October 7th massacre to appeal to “stop walking on eggshells, afraid of what people will think. Let them call it terrorism. Extremism. Barbarianism. We call it liberation. Decolonization. Resistance. Revolution.” NYU Langone Winthrop Hospital thankfully disagrees with WC4BL and called the statement grounds for termination.
Abeer AbouYabis, a physician at Emory Winthrop Cancer Center, was investigated and ultimately fired for several pro-Hamas statements, including “They got walls we got gliders glory to all resistance fighters.” What precisely her employer needed to investigate is unclear, but none of it matters as far as WC4BL is concerned.
As Sally Satel chronicles in a recent Commentary piece, WC4BL has been signal boosted by the Association of American Medical Colleges and recognized as a resource for “antiracism” efforts. While WC4BL might be a good resource for defending terror apologia issued through the press organ of the Revolutionary Maoist Coalition, medical institutions interested in fighting rather than elevating bigotry should seek guidance elsewhere.
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_252966943-scaled.jpg17392560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-15 02:51:282026-02-11 15:33:39White Coats for Black Lives breaks their silence to demand apologies for terrorist sympathizers
Vituity, a healthcare staffing company, has an odd solution for improving patient health: Blatant racial discrimination. The proof is its new sponsorship of a racist scholarship for the Society of Hospital Medicine.
The scholarship is dedicated to advancing “diversity, equity, and inclusion,” with a special focus on “eliminating health disparities for hospitalized patients.” Naturally, it’s only available to applicants who are “underrepresented in medicine.” That’s a nod to minorities, and it’s a clear-cut case of racial discrimination.
Figure 1. Society of Hospital Medicine scholarship page.
Not only is discrimination wrong, but the operating assumption behind this scholarship is false. Activists claim that recruiting more minorities into the medical profession will help reduce health disparities between white patients and minority patients. Why? Because having more minorities in the medical profession will allow physicians and patients to be matched by race. This is called “racial concordance,” and it’s one of the top goals of woke activists.
Yet as Do No Harm has shown, “racial concordance” has no benefits. Studies show that it doesn’t improve health outcomes or decrease disparities. In fact, it’s more likely to harm patients by encouraging lower standards for medical professionals. It also lays the groundwork for the return of racial segregation. No one would tolerate white patients asking to be paired with white doctors. Why should woke activists get away with trying to match black patients with black doctors?
Vituity and the Society of Hospital Medicine should be ashamed. They’re supporting discrimination and paving the way to medical resegregation. This scholarship needs to end – and so does the woke misinformation that led to its creation in the first place.
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_361382480-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-10 13:18:042026-02-11 15:33:39Sorry, Vituity: Discrimination and Segregation Are Wrong.
The Thoracic Surgery Foundation is the latest medical organization to engage in racial discrimination. A source pointed us toward several concerning scholarships for 2024. Like so many other institutions in medicine, the Foundation is downplaying merit in favor of skin color, which ultimately puts patient health at risk.
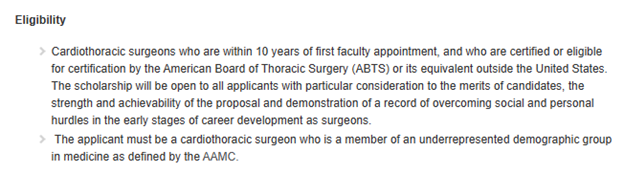
The scholarships in question are the “Underrepresented Robotic General Thoracic Surgeon Development Award” and the “The Levi Watkins Innovation and Leadership Development Scholarship.” Both are only available to applicants who are “underrepresented” in medicine. That’s code for racial and ethnic minorities whose representation in the medical profession is less than their share of the national population. It’s also blatant discrimination.
Figure 1. Eligibility criteria for the Levi Watkins Innovation and Leadership Development Scholarship.
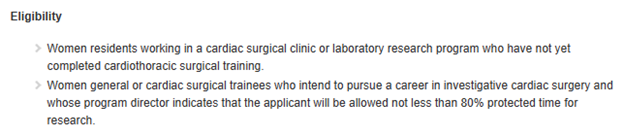
Several other scholarships are cause for concern. The “Nina Starr Braunwald Research Fellowship Award” is only available to female applicants, which is another form of discrimination. And the “AstraZeneca Reversing Health Disparities in Lung Cancer Research Award” is reviewed by the DEI committee, indicating the race-focused nature of the scholarship.
Figure 2. Eligibility criteria for the Nina Starr Braunwald Research Fellowship.
What possible justification is there for racial discrimination? Activists claim that recruiting more minorities into the medical profession will improve health outcomes, since it will help more patients connect with physicians of the same race. Yet as Do No Harm has shown, such “racial concordance” is not supported by evidence. It’s more likely to harm patients by encouraging lower standards for admission to medical school. It also lays the groundwork for the return of racial segregation.
The Thoracic Surgery Foundation shouldn’t be discriminating by race or gender. It’s immoral, insulting, and it will ultimately injure patients. Now when will the foundation put equality, merit, and excellent medical care first?
Does your professional organization offer scholarships or fellowship awards that contain discriminatory eligibility criteria? Please let us know via our secure online portal.
https://donoharmmedicine.org/wp-content/uploads/2023/07/shutterstock_1846708057-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-09 18:34:562026-02-11 15:33:39Discrimination Comes To Thoracic Surgery
The University of Wisconsin System recently announced it will use $32 million from state budget funds to expand healthcare training in the state. However, Wisconsin State Assembly Speaker Robin Vos has stated that no money will be released until the UW System eliminates all DEI initiatives.
Read the letter Do No Harm chairman Dr. Stanley Goldfarb sent to Speaker Vos, asking him to give special consideration to removing DEI in the medical education programs at UW. “This issue goes well beyond the quality of the education they provide,” Dr. Goldfarb said. “Ultimately, it affects the health and well-being of everyone who will one day be treated by the physicians, nurses, and other healthcare professionals they teach.”
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_1537717520-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-09 18:21:232026-02-11 15:33:39Dr. Stanley Goldfarb Recognizes Wisconsin State Assembly Speaker Vos for Stance Against DEI in Medical Education
Should medical schools force students or faculty to believe in “diversity, equity, and inclusion”? For that matter, should any institution of higher education? The obvious answer is a resounding “no,” yet federal law isn’t so clear. So kudos to Rep. Greg Murphy from North Carolina for fighting to enshrine fairness and free speech in the laws of the land.
Rep. Murphy, who’s a licensed doctor, recently introduced an amendment to the appropriations bill for Labor and Health and Human Services. The short amendment reads:
“None of the funds made available by this Act may be provided to a public institution of higher education that conditions admissions to any student applicant, or the hiring, reappointment, or promotion of any faculty member, on the applicant or faculty member pledging allegiance to or making a statement of personal support for or opposition to any political ideology or movement, including a pledge or statement regarding diversity, equity, and inclusion, or related topics.”
This amendment is needed because medical schools and other institutions of higher education are doing exactly that. To choose just one example: The Indiana University School of Medicine requires all faculty seeking promotion or tenure to submit a so-called “DEI Statement.” These statements show the faculty member’s commitment to this divisive and discriminatory ideology. It’s a blatant political litmus test, gutting free speech and corrupting medical education in service to a political belief system.
Many if not most medical schools (along with colleges and universities) now require similar DEI statements from faculty, staff, and/or students. If an institution of higher education is going to engage in this infringement on free speech, they shouldn’t receive taxpayer money. Rep. Murphy should be praised for championing this commonsense policy.
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_2108769203-1-scaled.jpg17122560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-09 17:57:522026-02-11 15:33:39Rep. Murphy’s Fight For Fairness and Free Speech In Congress
There are many misunderstandings about aspects of diversity, equity, and inclusion (DEI) and how it affects issues like civil rights, school accreditation, and the maintenance of DEI departments in higher education.
Read about five myths related to DEI and the facts that you need to be well informed about what DEI is, and what it isn’t.
https://donoharmmedicine.org/wp-content/uploads/2023/04/DNH_mocks_contentimages_Resource.png6751200Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-09 17:31:512026-02-11 15:33:39Myths and Facts About Diversity, Equity, and Inclusion (DEI)
The University of Kansas Medical Center School of Medicine (KUSOM) is requiring students to meet “diversity objectives and competencies” through assignments that demand a focus on “social determinants to health,” including patient claims of having experienced “systemic racism,” say Freedom of Information Act (FOIA) documents obtained by Do No Harm.
Even following the Supreme Court’s ruling in June that found race-based admissions practices to be unconstitutional, the Office of Diversity and Inclusion (ODI) at KUSOM is touting its dedication “to recruiting, retaining and promoting diversity and health equity among its students and faculty.”
Figure 1. Statement from the KUSOM’s Office of Diversity and Inclusion.
“Health equity” is a narrative of diversity, equity, and inclusion (DEI) ideology, which, based in Critical Race Theory (CRT), claims “systemic racism” and “oppression” prevent minority individuals from obtaining health care. According to the radical dogma, achieving “health equity” is dependent upon a “diversity” of races and ethnicities in the healthcare workforce.
Through its focus on DEI practices, KUSOM claims it “will become a national leader in inclusive excellence and health equity by purposefully mirroring the communities that we aspire to partner with and serve.”
As part of a Family Medicine Clerkship, for example, KU medical students are required to interview a patient facing a “social determinant to health,” a politicized label that places “mental health issues” and “physical disability” in the same category as “experiencing bias based on race, religion, gender, etc.”
The patient interview, the objectives say, can be conducted on “someone who has experienced stigma, negative stereotypes, discrimination, or violence based on religion, race, ethnicity, gender, sexual orientation, age, body size, physical or systemic powerlessness, medical or mental health problems.”
The assignment and samples of patient “stories” appear to serve the goal of creating an emotional impact on the medical students.
For example, the interview task requires medical students to turn in a “first-person voice” description of the patient they have interviewed – so that students must write the description as if they are the patient; a personal reflection of how the interview might “influence your future feelings, thoughts, or practice;” and a “power point slide with a meaningful visual image,” such as a “work of art, a symbol, a sports team, a building, or any image that enriches the story and enhances its memorability or emotional impact.”
Another diversity objective and competency requires the provision of “a forum for critical thinking about moral, cultural, legal, financial, and social issues in clinical medicine.”
The documents also indicate competencies required for graduation include:
a. Students will be able to incorporate social determinants of health to promote patient education and enablement of wellness regardless of patient or population based needs
b. Students will appreciate the influence of social determinants of health in various populations
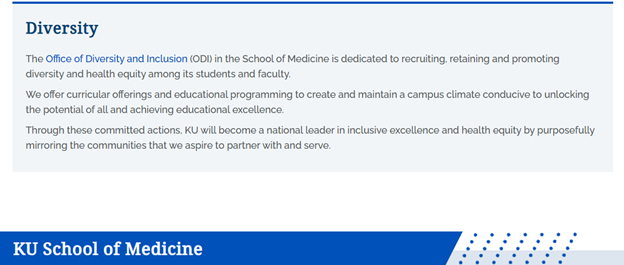
A KUMC document titled “Curriculum Diversity Thread Objectives” states Year 1 medical students must meet a goal of “build[ing] a shared language around structures that promote inequity, their effects on health, and frameworks for exploring health outcomes.”
Figure 2. From “Curriculum Diversity Thread Objectives” at KUMC.
Students must be able to “define race, ethnicity, and culture, and their implications on health and health care;” to “explain why race is a social construct and the implication for racialized medicine and health outcomes;” and “define Health Disparity/Inequality.”
The “diversity objectives” also require students to define “structural vulnerability, intersectionality, structural violence and structural racism.”
Year 1 students must also be able to “identify the processes through which inequality is naturalized,” and examine “culture/stereotypes, individual implicit bias,” and “institutional bias.”
The influence of CRT on medical education continues at KUMC as Year 2 students are required to “understand and use” a “structural competency framework as a tool to unveil the influences of structures that promote inequity on patient health and healthcare practice.”
In Years 3 and 4, medical students at KUMC are required to identify and “imagine” structural “interventions,” i.e., be able to use the “tools” that allow doctors to “take action to address health and illness as the downstream effects of broad social, political, and economic structures.”
KUMC makes clear a primary focus of its CRT-inspired medical training is a thorough understanding of “inequity,” “structural racism,” and “social determinants to health.”
“Diversity is good, but it should never come at the expense of quality,” Do No Harm Chairman Stanley Goldfarb, M.D. warned, however, at National Review in October.
He explained while many minority individuals are highly qualified for admission to medical schools, still “a great many aren’t,” and “yet the powers that be are lowering standards to let them in.”
The Supreme Court has ruled that race-based admissions policies and practices are unconstitutional. Despite the fact that “poor academic performance in medical school is a predictor of poor performance in post-graduate clinical training,” Goldfarb nevertheless observed that “medical schools are still looking for ways to prioritize race and gender over academics.”
https://donoharmmedicine.org/wp-content/uploads/2022/08/shutterstock_1888448323-scaled.jpg17062560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-09 13:33:492026-02-11 15:33:39University of Kansas School of Medicine Requires Students Complete ‘Social Determinants to Health’ Assignment to Meet DEI Objectives
Nashville, TN; November 8, 2023: Today, Do No Harm, a prominent national nonprofit committed to safeguarding healthcare from radical and divisive ideology, filed a federal lawsuit against the unlawful racial quotas imposed on the governor of Tennessee when making appointments to state boards and commissions.
The Tennessee Board of Podiatric Medical Examiners requires one board member to be a racial minority, which has nothing to do with podiatry. A seat reserved for a racial minority opened in June 2023, and despite no shortage of qualified podiatrists in Tennessee, the governor has not made any appointments to the board.
“State medical boards are given important responsibilities to oversee the quality of care in their state and the safety of patients. It is crucial that they be the most qualified physicians available. Like all aspects of healthcare, patient safety and patient concerns should be primary, not the skin color or the racial makeup of any oversight committee,” Dr. Stanley Goldfarb, board chair of Do No Harm.
“Tennessee law forces governor after governor to engage in racial discrimination when making appointments to state boards and commissions,” said Laura D’Agostino, an attorney with Pacific Legal Foundation who are bringing the suit pro-bono. “Using race to make appointments to government boards is not only demeaning and unconstitutional, but it undermines the distinctive spirit of the Volunteer State by precluding opportunities for Tennesseans to serve their local communities.”
Tennessee is far from the only state that uses immutable characteristics to limit opportunities for individuals to serve their state and local communities. A report released by PLF, Public Service Denied, found that 25 states codify such unconstitutional discrimination.
The case is Do No Harm v. William Lee and was filed in U.S. District Court for the Middle District of Tennessee. Find additional information here.
###
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. With more than 5,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and in 14 countries, DNH has achieved more than 4,900 media hits in top-tier publications and garnered widespread attention through numerous broadcast news appearances.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200rededge-rachelhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngrededge-rachel2023-11-08 19:56:252026-02-11 15:33:39Do No Harm Challenges Tennessee’s Racial Quotas for State Boards and Commissions
Clinical Advisor claims to be a medical news and opinion site designed for nurse practitioners and physician assistants. Discerning whether that news is real or fake will require some effort from readers.
A recent article offered up an intriguing headline: “Cultural competency training changes behavior among emergency department nurses.” The headline references a poster presentation at the recent DNPs of Color Annual Meeting. The poster shares results from an intervention in which the researcher measured “cultural awareness” at baseline, then once again immediately after watching a one-hour movie called “Ending Racism is Everyone’s Responsibility,” and then a third time four to six weeks after that. The researcher observed that “cultural awareness” scores increased through the three observation periods.
According to the researcher, “the data revealed a behavioral trend and clinical significance.” That characterization is inaccurate for several reasons.
First, experiments must include intervention and control groups to parse out treatment effects from other factors that could shape the outcomes of the intervention group, such as placebo effects (i.e., benefits that arise from the participant’s belief that the intervention is effective) or Hawthorne effects (i.e., participants altering their behavior because it is being observed by researchers). It is entirely possible that the survey responses of the participants changed because they were mindful of being observed or that they hoped for the intervention to succeed.
Second, attitudinal surveys are not indicative of “behavioral trends.” Surveys and tests are often poor predictors of human behavior, including issues related to race. The popularly utilized Implicit Association Test, which is used to measure “implicit bias,” does not demonstrate any ability to predictracist behavior. Most likely, the survey trends observed in this “study” do not equate to behavioral changes, and indeed it strains credibility and common sense that watching a one-hour video would alter patterns of human behavior.
Third, the claim the results were “clinically significant” is a matter of personal judgement, and one that is contradicted by the objective measure of statistical significance. In fact, the reported statistical significance—a measure that determines the likelihood that the results were determined by some effect rather than random chance—doesn’t even come close to reaching conventional thresholds of significance.
The study and its characterization in Clinical Advisor are emblematic of a healthcare establishment that continues to embrace the pseudoscientific claim that racism permeates American medicine, and the equally dubious idea that it can be expunged through interventions with no history of success. Evidence for these ideas is wanting, even if Clinical Advisor pretends otherwise.
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_2292867633-scaled.jpg16002560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-07 15:11:572026-02-11 15:33:39Clinical Advisor is Misadvising
In 2018, Raheem Williams couldn’t have known that his professional and educational backgrounds in economics and social policy — combined with a personal history of digging for medical answers — would lead him to be an advocate for the safety of children.
But today, Williams is just that: A researcher who demands data-driven information about all things, especially when it involves children and irreversible medical procedures.
A practiced researcher and policy analyst by trade, Williams began noticing something while digging through medical jargon and empirical research on Google Scholar: Medical news reports were ablaze with mentions of youth “gender affirming care,” “life-saving care,” and “gender ideology.” Williams’ propensity for research told him to dig deeper past the buzzwords. He didn’t like the narrative that he saw.
“For roughly four years, I was a silent observer, just reading and watching the narrative unfold. But I noticed that the language used by medical professionals and the media was trying to equate transgender youth to gay rights—but fundamentally, it’s not. Challenging the notion of putting kids through medical procedures that are lifelong and completely elective isn’t about gay rights. It’s about one question: Can kids consent?” Williams said.
“When you see bad things happening and no one speaks up, it gets worse. I was—and am—fundamentally bothered by the lack of conversation around this issue and the way the media purposefully uses language that misleads people, like ‘life-saving care.’ Most Americans don’t understand that this is a dog whistle for radical policies. I felt compelled by the basic issue of human decency to speak up.”
Raheem Williams, Do No Harm senior fellow.
Williams’ background in policy and his expertise in research has allowed him to speak on the issue of transgender youth in a way that few can command. Williams finds it particularly disturbing that what medical practitioners and scientists are saying to each other behind closed doors is miles apart from what they’re telling the public. His paper, The Trans Youth Phenomenon: Critiques and Hard Questions, forces readers to confront the medical evidence that points out that there is no biological basis for transgender ideology, and what little evidence that does exist raises new ethical dilemmas, particularly among children and the use of puberty suppressors.
But that research is ignored by the media, activist clinicians, and advocates so-called “gender affirming care” who instead promote weak research to justify their worldview.
“There’s a universality in public policy where Americans tend to be indifferent to problems that they don’t see as their own. With lawmakers, we need to zoom out,” Williams said.
“It’s a fundamental question: What exactly is a minor? Why do we have legal protections for minors? That’s what we need to think about right now. I live in a country where you must be 21 to buy cigarettes but I’m being told that even a 12-year-old can understand the ramifications of a sex change.”
That question is one Williams is determined to have every adult answer as he advocates for the victims — kids and their parents alike.
“As a society, we must get back to protecting the innocence of children. Where we, as adults, understand the extreme difficulty of making serious decisions and do not put that burden on kids,” Williams said.
He is quick to empathize with parents who truly believe they are protecting their children by advocating for them — parents who have been told over and over by medical professionals that their child needs to transition, lest they kill themselves. According to Williams, these parents are victims too — victims who deserve honest practitioners.
Williams believes the more our society lifts the voices of these victims, the more the public will understand this issue — and combat it. His experience testifying in the states has shown him that people on both sides of the political aisle, across every religion, creed, and skin color are opening their eyes to the gravity of this issue, and the lasting ramifications it has on our children. New groups of people are coming together and discovering they have one thing in common: Common sense — and the desire to protect kids.
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_388660693-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-06 16:31:002026-02-11 15:33:39Meet Raheem Williams, Do No Harm Senior Fellow
Washington State University’s Elson S. Floyd College of Medicine doesn’t want to reveal just how much it has aligned with the AAMC’s politicized policies for medical schools, as it has shown in its Diversity, Inclusion, Culture, and Equity (DICE) Inventory document it sent to Do No Harm.
Here’s the background. In November 2022, the Association of American Medical Colleges released a report showing that the vast majority of medical schools have embraced identity politics, despite their divisive and even discriminatory nature. The report was based on surveys of specific medical schools, which the AAMC didn’t name.
For the sake of transparency and accountability, Do No Harm submitted freedom of information requests to public medical schools nationwide, including Washington State University College of Medicine (WSUCOM). We asked for a copy of its DICE Inventory survey response, so that Washington taxpayers and policymakers could learn the truth about this institution.
However, WSUCOM was unwilling to provide a complete version of the Excel spreadsheet that participating schools sent to AAMC. In April, the school sent an Excel document titled “22-436 Installment No Redactions.xlsx.” But upon review, the spreadsheet has had all the comments columns removed. For example, here is how the Government, Leadership, & Mission tab should appear (there is a column on the right titled “Supporting Evidence – Free Responses” that is available for the school to enter comments):
Figure 1. Except from the AAMC’s DICE Inventory Excel spreadsheet.
This is how the same tab (and all the tabs) of the Excel spreadsheet sent by WSUCOM appears (note how the column for “Supporting Evidence – Free Responses” is missing):
Figure 2. Excerpt from the WSUCOM DICE Inventory Excel spreadsheet.
Upon questioning the Public Records Office at WSU, we were told, “The Office of Public Records did not delete or redact anything from the record. We also verified with the department that provided the record that they did not delete anything from the record prior to submission to the Office of Public Records.” Yet, the comments have mysteriously disappeared from the spreadsheet, which is something we haven’t seen in other cases.
Minus the comments – which were submitted in all other DICE Inventory Excel documents we received – here’s what the Washington State University College of Medicine has self-reported:
It has adopted racially discriminatory admissions practices under the guise of “affirmative action.”This means it’s potentially lowering standards in the name of diversity, thereby threatening patient health. An example is the “holistic admissions” process, which WSUCOM openly promotes: “Personal stories, reflection, and life experiences review what academic metrics cannot,” the schools Admissions Requirements webpage states.
It has a “dedicated office, staff, or resources”dedicated to DEI. This means there’s a permanent woke bureaucracy pushing ideology on faculty and students. In fact, WSUCOM is so dedicated to this agenda that it posts a 57-page “Strategic Diversity Action Plan” on its DEI office’s website.
It lobbies for woke policies at the federal, state, and/or local levels.This means it’s wading into toxic public debates instead of fully focusing on educating future physicians. “As WSU administrators and faculty continue to develop the medical school,” the Strategic Plan page states, “they stay in touch with the universities government affairs office, which maintains regular contact with elected officials who can provide resources to help the college.”
It offers tenure and promotion to faculty who prove their commitment to extreme identity politics and woke priorities.This is a litmus test that requires faculty to toe the party line instead of teaching medicine at the highest level. In its Guidelines for the Tenure and/or Promotion of Pre-Tenured and Tenured Facultydocument, WSUCOM notes that “efforts to promote diversity” are important for applicants to document when describing their service activities.
Its administrators are active within local, regional, and national forums to promote equity, diversity, and inclusion.This means it’s wasting resources that would be better spent on real medical education. The WSUCOM Student, Staff, and Faculty Resourcespage illustrate its alignment with the DEI position of the AAMC and with intercampus initiatives such as the Equity Committee.
All told, WSUCOM has instituted 89.5% of the divisive and discriminatory woke policies listed by the AAMC. And you can bet it is feeling pressure from activists and outside groups to go even further down the radical rabbit hole – doing even more damage to faculty, medical students, and ultimately, the millions of patients they’ll see.
Figure 3. WSUCOM DICE Inventory overall score.
Washington taxpayers help fund the Elson S. Floyd College of Medicine at Washington State University. They, and the policymakers who represent them, should ask why they’re giving so much money to an institution that’s putting divisive and discriminatory ideology at the heart of medical education.
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_592324490-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-04 12:13:232026-02-11 15:33:39Washington State University Hides Its Comments to the AAMC in the DICE Inventory