On February 1, I provided testimony to the Kansas State Legislature’s House Health and Human Services Committee (HHHSC) to present Do No Harm’s position opposing the radical ideologies based on diversity, equity, and inclusion (DEI) and anti-racism that have infiltrated medical education and the healthcare industry. But some members of the HHHSC were not willing to consider the objective facts that informed my presentation, and criticized them in a confrontational manner.
The main points of my testimony centered on how people are being seen and treated as groups – rather than as individuals – as a result of the divisive and destructive policies applied to medical education and patient care:
Workplaces and some state licensing boards use political ideology to determine how medical personnel are accepted into their organizations and how they will progress through their careers (e.g., requiring implicit bias training as a condition of employment or licensure).
Disparities in healthcare outcomes do exist; but they are largely due to poor access to care, not systemic racism or bias on the part of the patient care staff.
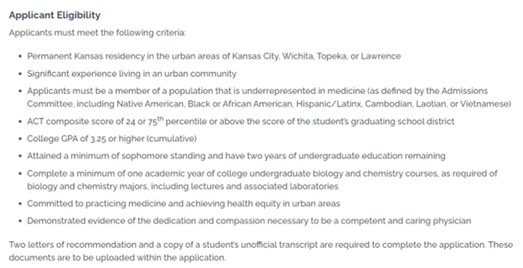
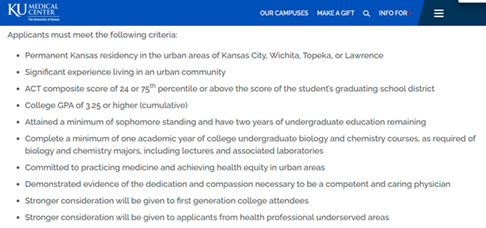
Procedures for acceptance into medical school are sacrificing achievement and merit in the name of diversity. Healthcare education is different in that, along with the school and the student, there is the need to consider what is best for the patient. The University of Kansas (KU) School of Medicine’s Urban Scholars program, which guarantees acceptance into the MD program upon completion, is an example of how certain groups of students are given preferential consideration instead of evaluating individual applicants on their academic achievements and qualifications.
Discriminatory practices have taken place in some healthcare institutions that are treating patients as groups instead of tailoring their treatment plans according to their individual needs. Healthcare providers are asked to view patients from a racial perspective instead of a clinical one.
After my 10-minute address about the effects of these DEI and anti-racism ideologies on the medical profession, there were some thoughtful questions posed by committee members who were seeking clarification on a particular point. However, not all the legislators were interested in engaging in a meaningful dialogue.
One member of the committee said he was “deeply offended” by my presentation and claimed that Do No Harm “advocate[s] for racist policies and practices” because of our stand against the concept of anti-racism. I explained that Ibram Kendi clearly communicates the intent of anti-racism when he states, “The only remedy to past discrimination is present discrimination. The only remedy to present discrimination is future discrimination.” The representative moved on to the issue of infant and maternal mortality in Kansas, but refused to reflect on the scientific literature. The evidence shows how a lack of early prenatal care and reliable access to facilities that can care for patients with severe maternal complications contributes to this problem, not systemic racism in the healthcare industry. “We must be looking at different data,” he said. “I guess we’ll just agree to disagree.”
https://youtu.be/HnYuGMnmv_A
Similarly, the next representative insisted the cause of poor access to care “is arguably systemic racism.” Despite my rebuttal citing a lack of data to show that health disparities in minorities are due to bias on the part of healthcare providers, she reiterated that “DE&I and these sorts of practices are extremely important” to address them; otherwise, “it’s doomed to repeat itself.”
https://youtu.be/qOvSpVKhXnA
Another committee member asked me, “Why are you here, and what do you want from us?” I explained our proposal including the removal of DEI questions from the med school application process and education in divisive concepts like Critical Race Theory and anti-racism. Her recommendation was for Do No Harm to change its name, stating, “Your group is providing much more harm to the public.”
https://youtu.be/uL5h6Tq9KzU
Finally, a representative who is also a primary care physician mentioned the KU Urban Scholars Program in his questioning, which was quite argumentative. It was difficult to get an answer in, but he asked if my comments were based on what was seen on an internet site, which is correct. Do No Harm filed a federal civil rights complaint against KU Medical Center for racial discrimination in the eligibility criteria for this program, which were publicly visible on its webpages. Although this committee member described Urban Scholars as “a hallowed program” at KU, the Office for Civil Rights opened an investigation into it earlier this year as a result of our complaint, which demonstrated how KUMC was violating Title VI of the Civil Rights Act of 1964 by having race-based eligibility criteria for the program:
Here’s the takeaway from my experience in front of the Kansas HHHSC: This wasn’t an easy Q&A, and it demonstrates how the ideological left attacks ideas they don’t agree with, rather than being willing to engage in an informative and productive discussion. But, armed with the facts and evidence, it’s possible to pose a cogent and confident response in the face of confrontation and criticism. And, when discriminatory policies and programs are exposed, they can be corrected to align with federal law. Don’t let the confrontational tactics of the ideologues deter you from speaking out: Fight back with the truth.
Stanley Goldfarb, MD is the former associate dean of curriculum at the University of Pennsylvania Perelman School of Medicine and chairman of Do No Harm.
Full video of the Kansas State Legislature House Health and Human Services Committee session can be seen here.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1142921345-scaled.jpg25582560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-02-23 20:07:422026-05-06 11:12:44My Testimony to the Kansas House – And How the State Legislators Reacted To It