The Indiana University School of Medicine (IUSM) is at it again pushing more identity politics on faculty and staff, this time with an online learning course called Mitigating Unconscious Bias in Decision-Making.
Do No Harm has previously covered IU’s other woke offerings, such as a training module from the IU Office of Academic Affairs that instructed job search committee members to consider their “implicit bias” and “whiteness” in the course of evaluating applicants, rather than focusing solely on their experience and suitability for the position.
The new course on “unconscious bias in decision-making” is an additional offering on the same topic, but for a wider audience. IUSM employees and students were notified of its existence via email, which Do No Harm was made aware of by an anonymous source. Even individuals who are not affiliated with the university can enroll: “While this training is designed with academic medicine in mind,” the email noted, “the content can be applied to any setting.”
Promoted by the woke dean of IUSM
The training module opens with a message from Dean Jay Hess, who notes that understanding one’s own perceptions is a fundamental step in making everyone at IUSM feel supported and encouraged. “On multiple occasions when I was faced with a decision,” he claims, “my decision-making was in fact influenced by unconscious bias.” He even acknowledges that the training itself is questionable. “There is some research and there are many people out there who question the value of unconscious bias training,” he says. But he encourages it as “important” for IUSM from the perspective of recruitment, evaluation, and promotion of people, and even to the care of patients.
Figure 1. Course offered by the Indiana University School of Medicine.
Training places equity and justice at the center of patient care
The first unit of the module says that IUSM “commits to identifying and dismantling hate, oppression, systemic racism, and discrimination in academic medicine,” and instructs learners to do the same by taking steps to address diversity, equity, inclusion, and justice.
“As we become more aware of our biases, we can make better data-informed decisions,” said Dr. Alvaro Tori, associate dean for Diversity Affairs at IUSM. He also advised learners regarding “taking inventory of the identities that you ascribe to and the power, privilege, and oppression that we each navigate.” Dr. Tori said that these measures place equity and justice in the center of the work of patient care, education, and research.
Subsequent sections in the training provide a roadmap for taking such an identity-based inventory and buying into the concept of “equity.” Units 2 and 3 in the module used YouTube videos, created by the University of California Los Angeles (UCLA) in 2019, with the ubiquitous explanation of biases being our brains’ way of taking shortcuts to deal with information overload and numerous examples of types of bias.
https://youtu.be/BwYFhJO9t50
Video from “Mitigating Unconscious Bias in Decision-Making” at IUSM.
In Unit 3, the Implicit Association Test (IAT) is introduced, and despite its weak science, the module content states “the IAT is considered more reliable and valid than survey evaluations.”
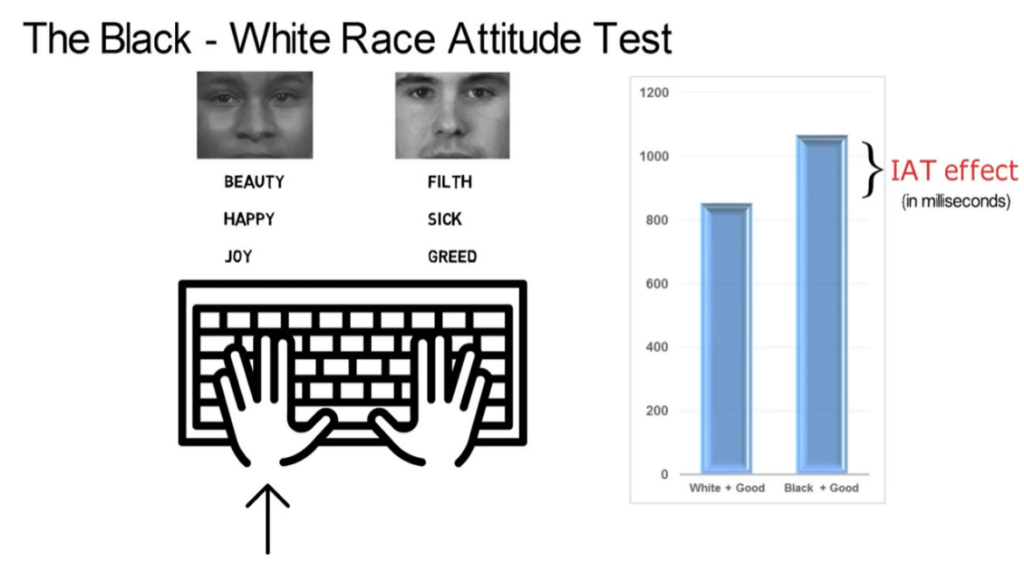
But it goes to the extreme in an effort to make its misguided point. The UCLA video on this topic refers to “The Black-White Attitude Test,” and describes how the tester will see pictures of a young black male’s face and a picture of a young white male’s face. The tester is instructed to sort the faces by hitting a key on the left side of the keyboard for white, and key on the right side for black. The next step is to sort words in two “attitudinal categories” using the words “beauty,” “happy,” and “joy” or “filth,” “sick,” and “greed.” The tester then identifies the “good” words by striking a key on the left, and the “bad” words using the right side of the keyboard. The final step is to sort the words and the faces together. However, the exercise further conditions the tester to associate positive words with white faces and negative words with black faces by actually instructing him or her to do so. The narrator states that when good words are associated with white faces and bad words are associated with black faces, “you will find your groove and fly through this test. Most of us do.”
Figure 2. From “Lesson 5: The IAT” from the UCLA Office of Equity, Diversity, and Inclusion (a component of the IUSM Mitigating Unconscious Bias course).
However, when the procedure is reversed, the claim is that the process takes longer and testers will make more mistakes. The video attributes this to the so-called “IAT Effect,” which “reflects the strength of an attitude” and indicates “an implicit preference for whites.”
https://youtu.be/hr9xAcWv790?t=135
Video from “Mitigating Unconscious Bias in Decision-Making” at IUSM.
There is no proof that unconscious bias plays a role in clinical decision-making that leads to disparate outcomes. Beyond the fact that the IAT fails in its goals, there simply is no evidence that using it is beneficial in any way.
IUSM’s training offers conflicting advice
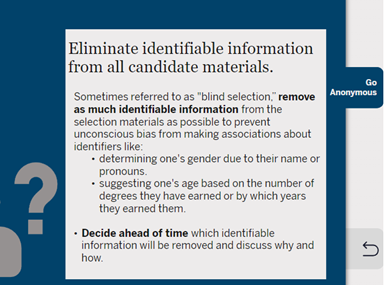
Unit 3 offers a discussion of the ways to address individual bias. The material moves into the “group mitigation strategies” and a section that describes “What We Will Do.” One of the strategies is to “go anonymous,” meaning that any information that could be used to identify an individual is to be eliminated from application documents, thus creating a “blind selection” process.
Figure 3. From “Mitigating Unconscious Bias in Decision-Making” at Indiana University School of Medicine.
But that doesn’t align with the IUSM Office of Academic Affairs training module, which makes it clear to search committee members that they are to use “equity benchmarks” at every point of faculty candidate review and selection (emphasis added):
Here are some strategies that serve to buffer outcomes from the impact of bias. First, search committees should adopt an inclusive mindset. Rather than trying to narrow the pool down, they should try to make it as inclusive as possible. Furthermore, at each point of the process that the pool gets narrowed, the committee should ensure that the percentage of minoritized applicants continues to reflect the percentage in the original pool. If it does not, then the committee might revisit their criteria for evaluating applicants. Second, establish and use well-defined criteria to guard against bias. As we discussed, criteria that seem valid on the surface may systematically disadvantage applicants of color. Wherever possible, eliminate biased metrics or find ways to adjust for them in the ratings. Finally, ensure accountability by agreeing that decision-making processes must be clear to all committee members and by slowing down the evaluation process so as not to rely on biases and heuristics when assessing candidates.
So what are IUSM community members supposed to do? Anonymize data, or insert percentage controls of minoritized applicants? It is no wonder that Do No Harm has heard from so many concerned stakeholders who feel that they’re being fed contradictory guidance that constantly pushes identity politics.
It’s time the Indiana University School of Medicine stops wasting time and resources on training that only serves to create division. State policymakers are starting to pay attention to constituent requests for help to force some sanity back into the school.
Is your school or healthcare organization requiring implicit bias training? Please let us know via Do No Harm’s secure online portal.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1244076769-scaled.jpg17092560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-09-05 21:44:302026-05-11 14:48:27The Indiana University School of Medicine Just Can’t Get Enough of Woke Ideologies