Boston Medical Center currently maintains on its website the “Glossary for Culture Transformation” (“the Glossary”), an exhaustive list of terms referring to various tenets of DEI ideology. Examples include “anti-racism,” “privilege,” “Latinx,” and many, many others.
As the Glossary webpage makes clear, these terms are intended to advance the DEI goals of Boston Medical Center, Boston University Medical Group, and related educational institutions.
Here’s how the Glossary webpage describes the creation of the Glossary:
“The Office of Equity, Vitality, and Inclusion, in partnership with Boston Medical Center, Boston University Medical Group, Boston University Chobanian & Avedisian School of Medicine, Boston University School of Public Health, Boston University Goldman School of Dental Medicine, and Boston University Graduate Medical Sciences collaboratively developed this Glossary as a tool to align our goals of justice, equity, and belonging and strengthen our collective understanding. Establishing shared language is foundational to creating common understanding by expanding our awareness of the world beyond our individual identities and experiences.”
So, in other words, all of these clinical institutions are culpable for injecting radical identity politics into healthcare through the Glossary.
The definitions of these terms are further evidence of this ideological goal.
For instance, the definition of “anti-racism” is sourced explicitly from Ibram X. Kendi, a radical proponent of racial discrimination on the basis of remediating past injustices.
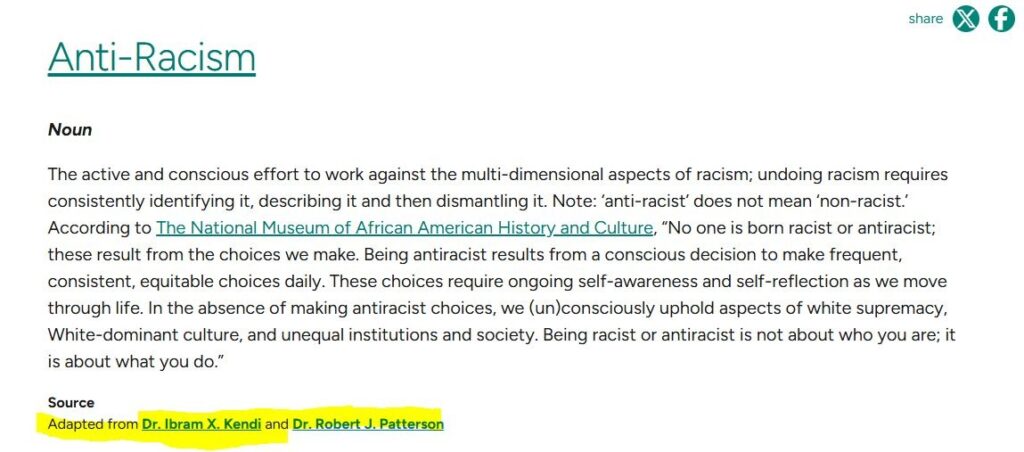
“The only remedy to past discrimination is present discrimination,” Kendi has said. “The only remedy to present discrimination is future discrimination.”
It’s also worth noting that as recently as January 2025, Kendi maintained a research center at Boston University.
The definition of “privilege,” meanwhile, falsely states that “White people in America are privileged in that their race will not limit their economic or educational prospects.”
Yet, Do No Harm has documented countless instances of medical schools explicitly excluding white and/or Asian students from educational opportunities on the basis of race.
And in medical school admissions, white and Asian students often face much longer odds of admission than their black and Hispanic counterparts with equivalent GPAs and MCAT scores.
Indeed, the Glossary contains several terms that appear laudatory of efforts to engage in racial discrimination.
The definition of “racial justice” reads as follows: “The creation and proactive reinforcement of policies, practices, attitudes, and actions that produce equitable power, access, opportunities, treatment and outcomes for all people, regardless of race.”
It should go without saying that any attempt to equalize “outcomes” among racial groups will invariably involve favoring some racial groups over others. Many such discriminatory policies are even justified under the guise of health equity or similar concepts.
Other entries are more overtly political.
The entry for “decolonization” includes a definition of decolonization as “the active resistance against colonial powers, and a shifting of power towards political, economic, educational, cultural, psychic independence and power that originate from a colonized nation’s own indigenous culture. This process occurs politically and also applies to personal and societal psychic, cultural, political, agricultural, and educational deconstruction of colonial oppression.”
What this has to do with Boston Medical Center’s (ostensible) goal of providing the best possible medical care is anyone’s guess. It seems instead to be evidence that Boston Medical Center is content to serve as a vehicle for radical political activism, at the expense of a focus on clinical excellence.
What’s more, as the Glossary’s webpage states, “the Glossary for Culture Transformation is a living document to be revised on an annual basis.”
If that is indeed true, then Boston Medical Center has been doubling down on its commitment to radical ideology.
Hopefully, it will rediscover fundamental principles of medical ethics – to strive to “do no harm” and provide the best possible care – and ditch identity politics for good.