Salt Lake City, UT; January 27, 2026 – Today, Do No Harm released a report entitled “Debunking Frakes and Gruber’s New Study on Racial Concordance.”
The report refutes a recent study, authored by economists Michael Frakes and Jonathan Gruber, that misleadingly claims racially diverse military medical facilities improve care for black patients. However, the study fails to actually examine whether black patients have better outcomes when treated by black doctors, and buries a key finding that undermines the thrust of the study’s conclusion.
Frakes and Gruber instead offer two flawed explanations for the study’s claims: 1) black doctors teach their peers how to better connect with black patients, and 2) the presence of black doctors in hallways increases black patients’ trust in non-black providers.
“We cannot allow politically motivated activists to push debunked racial theories that have no positive impact on patient care,” said Jay Greene, Director of Research for Do No Harm. “Studies like this are designed to codify DEI doctrine to pave the way for re-establishing affirmative action and enshrining race-based hiring. The report ignores the very question it purports to answer: whether black patients actually fare better with black doctors. Our report systematically exposes the study’s shoddy methodology and baseless conclusions. Americans of all races and backgrounds deserve high-quality medical research, not political ideology disguised as science.”
Flaws in the Frakes & Gruber Study:
The study never actually examines whether black patients fare better when treated by black doctors.
The study buries the finding that black patients actually do best when treated by non-black doctors in facilities that happen to have more black doctors, which undermines the claim that black patients need to be served by black doctors
The study not only relies on debunked research but also fails to cite systematic reviews that already found no evidence that racial concordance benefits patients.
Do No Harm’s report also notes that co-author Jonathan Gruber is infamous for bragging about relying on the “stupidity of the American voter” while helping mislead the public with opaque analyses to pass the Affordable Care Act.
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. It has over 50,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 14 countries.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2026-01-27 13:57:122026-02-11 15:34:19Do No Harm Report Debunks Prominent ‘Racial Concordance’ Study
A.T. Still University (ATSU) is offering a scholarshipthrough its Diversity Department ostensibly intendedto support “students who learn and serve in diverse, underserved, urban, and rural communities across the globe.”
The Graduate Health Professions Scholarship (GPS) promises recipients “significant financial support during their residential education.”
But the program description, while not explicitly limiting eligibility to applicants of certain racial groups (and even containing a non-discrimination disclaimer), contains some suspicious language. Additionally, the scholarship encourages recipients to engage in DEI activities.
First, the scholarship is intended to “attract and educate students whose life contributions and experiences are consistent with the ATSU mission to serve in underserved areas.”
This language in itself may seem benign, but consider the following context: the scholarship next includes a definition of “underrepresented minorities.”
“A. T. Still University defines ‘Historically Underrepresented’ and ‘Underrepresented Minorities (HUGs)’ as those persons identified by the Civil Rights Act of 1964 and the Health Resources and Services Administration (HRSA).”
The HRSA definesunderrepresented minorities as “American Indian or Alaska Native”; “Black or African American”; “Native Hawaiian or Other Pacific Islander”; and “Hispanic.”
Although the scholarship application criteria does not explicitly contain language discriminating on the basis of race or sex, it’s certainly alarming that the scholarship would include this definition at all, and it’s likewise unclear what purpose it serves.
And there’s a further wrinkle: per a brochurecontaining a list of scholarship recipients on ATSU’s website, none of the listed recipients appear to be white or Asian.
The scholarship also contains requirements stating that recipients are encouraged to participate in “campus-wide Diversity Department programs and initiatives,” and must “meet with [the] program administrator or [the] D&I (Diversity & Inclusion) representative at least once monthly.”
Needless to say, this is more than a little troubling, especially when viewed in conjunction with the other language in the program description.
ATSU should make clear that its scholarship is available to all, and ensure that it is not seeking to award the scholarship only to members of certain racial groups.
A non-discrimination disclaimer alone isn’t going to cut it.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1255382035-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2026-01-21 19:14:462026-05-14 16:02:08Medical School’s DEI Scholarship Is Cause for Alarm
Legislation introduced in Virginia this year could force healthcare professionals to endure ideological programming under the guise of combating “unconscious bias.”
One bill, SB 22, would require certain healthcare professionals to submit to “bias reduction training” in order to maintain their licenses.
Specifically, the bill directs “the Board of Medicine and Board of Nursing to require certain licensees to complete bias reduction training as part of their continuing education and continuing competency requirements for licensure.”
The legislation explicitly identifies “unconscious racial bias [that] affects care during pregnancy and the postpartum period” as a target.
This legislation is not new. Indeed, a very similar bill was introduced last year that also sought to target “unconscious bias”; then-Governor Glenn Youngkin vetoed the bill in May.
The notion that unconscious or implicit bias contributes to any real world impact is unsupported by solid evidence.
The tests used to evaluate or identify implicit bias fail to meet widely-accepted standards of reliability and validity and have beenfound to be “poor predictors” of real-world bias and discrimination.
And what’s more, Ohio State University psychology professor emeritus Hal Arkes describedthe test as “an extremely feeble predictor of behavior.”
It’s common sense that healthcare professionals should not be forced to undergo training grounded on false premises that accuses them of racism.
Virginia’s healthcare boards best serve their state when they focus on ensuring healthcare professionals adhere to standards of clinical excellence, and not when they inject dubious and divisive scientific concepts into healthcare education.
It’s also worth noting that SB 22 is just one of aflurryof billsintroduced this year that seek to advance DEI and related discriminatory practices within the Commonwealth.
These efforts are already attracting the attention of the Department of Justice’s Assistant Attorney General for Civil Rights, Harmeet Dhillon.
Given this scrutiny, it would be wise for state officials to avoid expensive lawsuits and ensure that taxpayer funds do not go toward the costs of defending racist laws.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2149875605-1-scaled.jpg13502560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2026-01-21 19:10:042026-05-14 16:03:43Virginia Legislation Would Subject Nurses to ‘Bias Reduction Training’
Dalhousie University in Nova Scotia, Canada, has adopted a new approach to pursue its goal of racial diversity in medicine: abandoning academic standards for black applicants altogether.
The Black Learners Admissions Pathway, a program with the ostensible goal of helping “facilitate entrance into the undergraduate medical education program for Black students,” requires black applicants no objective measures of academic achievement.
The program requires applicants to identify as either “Black/African Nova Scotian”; “Black/African Canadian”; “or Black/African.”
“There is no minimum grade point average (GPA) required under the Black Learners Admissions Pathway, but the Black Learners Admissions Subcommittee may use general GPA requirements as a point of reference during the holistic review process,” the program description states.
The Dalhousie Medicine Admissions Committeerequiresapplicants of other racial groups to have a GPA of 3.3.
Likewise, there is no minimum MCAT threshold for black applicants, though an MCAT score completed within the past 5 years is required.
“No MCAT thresholds are required for eligibility under the Black Learners Admissions Pathway but the Black Learners Admissions Subcommittee may use general MCAT requirements as a point of reference during the holistic review process,” the program description states.
The minimum MCAT scorefor applicants who don’t enjoy this exemption is 492.
Dalhousie operates a similar program for indigenous students as well: the Indigenous Admissions Pathway, in which MCAT scores are optional.
Meanwhile, applicants in the Rural Applicant Pathwayalso do not need to meet a minimum MCAT threshold, but still must meet the GPA requirements.
As mentioned above, the Black Learners Admissions Pathway is intended to “diversify the healthcare workforce by applying equitable admissions processes for Black learners.”
Of course, imposing one standard on certain racial groups and another standard on other racial groups is the opposite of fair: it’s textbook discrimination.
In the zero-sum game of medical school admissions, one applicant’s benefit is another’s burden. But more than that, admitting applicants who are definitionally less qualified will almost certainly degrade patient care.
Dalhousie cannot produce the best possible physicians when it explicitly seeks to recruit applicants who fail to meet minimum standards of academic performance.
Additionally, qualified black physicians may have to endure the perception that their admission to medical school was due to their race, and not their competence and merit.
Dalhousie should abandon its discriminatory practices and focus on providing the best possible medical education to all, no matter their race.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2054953619-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2026-01-21 13:40:192026-05-14 16:04:03Medical School Program Abandons Admissions Standards for Black Applicants
The Medical College of Wisconsin sent asurvey to its medical students intended to educate them about the effects of climate change on patient health, with a particular focus on nutrition.
The presentation accompanying the survey, titled “Climate Change, Gastroenteritis, and Malnutrition: What Physicians Should Know from the Inside Out,” discusses the various ways that “planetary health” can impact individual health, such as through pollution. Additionally, the presentation encourages students to get involved with climate activist groups.
The presentation contains the following learning objectives:
Understand that human health and planetary health are directly linked, and climate change is a public health crisis
Define climate justice and list populations most vulnerable to climate change
Describe how climate change is changing the distribution and increasing prevalence of vector borne gastrointestinal infections
Understand the impact of climate change on food security and associated nutrient deficiencies, particularly in vulnerable populations
Identify that plant-based diets are mutually beneficial to patient health and planetary health
A keen reader may have noticed that many of these objectives have very little to do with the practice of medicine and seem more geared toward an audience of policymakers in the public health sphere.
Indeed, the presentation encourages students to track their own “carbon footprint,” also discouraging the consumption of red meat for its comparatively higher impact on emissions.
How this prepares students to become the best possible physicians is anyone’s guess.
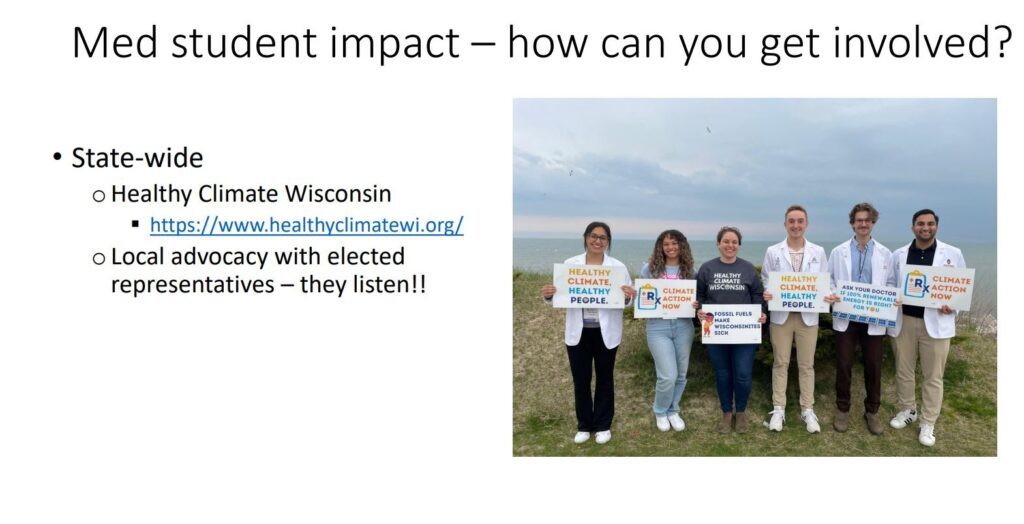
Next, the presentation outright encourages students to “get involved” with local activist efforts.
The presentation links to the websiteof Healthy Climate Wisconsin, a policy and advocacy organization that pushes for legislation and candidates targeting the oil and gas industry.
It’s also worth noting that Healthy Climate Wisconsin’s website includes an “Anti-Racism” webpagethat includes the following pledge: “We strive to make each of our working groups and each of our projects advance anti-racist ideals. By keeping Black, Indigenous, and People of Color at the forefront of climate action and transition plans we can help improve health disparities and create new economic opportunities for these vulnerable populations.”
That page also links to an articlecalling for racial discrimination in the distribution of vaccines during the COVID-19 pandemic.
The presentation even urges students to engage in “Local advocacy with elected representatives.”
It should be common sense that the classroom is not the appropriate venue for activist recruitment efforts, much less a venue for radical identity politics.
It is simply not the province of medical schools to instruct students on these issues.
Rather, this presentation is yet another example of increasing mission creep, where all sorts of political, social, and cultural activism are justified under the auspices of improving public health.
That the course encourages students to involve themselves in climate activism represents a significant straying from the actual purpose of medical education.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_308558309-scaled.jpg18152560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2026-01-21 13:18:452026-05-14 16:04:19Medical College of Wisconsin Pushes Students to Engage in Climate Activism
SALT LAKE CITY, UT; January 16, 2026 – The Department of Health and Human Services Office for Civil Rights (HHS-OCR) has re-opened a civil rights investigation into the Ohio-based Cleveland Clinic after a complaint was filed by Do No Harm and its legal counsel at the Wisconsin Institute for Law & Liberty (WILL). The complaintwas originally filed in August 2024; and while HHS-OCR initially opened an investigation into the Clinic, the matter was closed by the Biden Administration just days before President Trump took office.
Recently, the Trump Administration granted Do No Harm’s request for reconsideration and will re-open its investigation into the alleged discrimination at Cleveland Clinic.
Do No Harm’s complaint focuses on two specific examples of race discrimination at Cleveland Clinic: the Minority Stroke Program and the Minority Men’s Health Center. Both programs were specifically purposed for “preventing and treating [health conditions] in racial and ethnic minorities” through education, prevention, treatment, and other assistance and resources for addressing stroke and diabetes (and other stroke risk factors) as well as men’s health conditions and mental health issues.
Quotes:
“The Department of Health and Human Services is correct to revisit our complaint against Cleveland Clinic’s discriminatory programs and we welcome their efforts,” said Do No Harm Chairman Stanley Goldfarb, MD. “Injecting racial discrimination into treatment practices is unlawful, irresponsible, and leads to misunderstanding of disease and disease risk. Left unchecked, programs like the ones subject to our civil rights complaint erode public trust in medicine and will lead to worse health outcomes for all Americans.”
“Rather than treat all patients equally and provide care based on individual treatment needs, Cleveland Clinic unlawfully decided to allocate care and resources to certain patients because of their race,” said WILL Associate Counsel Nathalie Burmeister. “Now, there will be consequences. WILL is proud to work with Do No Harm in bringing true equality to the health care space.”
Additional Background:
Race-based health equity initiatives, like Cleveland Clinic’s programs, aim to filter and view health outcomes through a racial lens, assuming that one’s race says all the doctor needs to know about who needs medical care the most. However, beyond race, any number of demographic filters could be applied concerning almost any characteristic to compare and address health outcomes—to name a few, height, eye color, birth order, handedness, entertainment preferences, where one lives, etc. The availability of any particular demographic does not make it an appropriate, relevant, comprehensive, or lawful standard for evaluating and addressing health outcomes.
Cleveland Clinic’s race-based Minority Stroke and Minority Men’s Health Center programs ultimately seek to balance the scales of mortality and morbidity based on nothing more than bare reliance on a patient’s skin pigmentation. This interest in race for race’s sake is not only immoral, but also illegal.
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. It has over 50,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 14 countries.
Like many medical institutions, American Family Physician (AFP), the journal of the American Academy of Family Physicians (AAFP), fully embraced a commitment to radical identity politics in the wake of the “racial reckoning” of the summer of 2020.
For example, AFP and other family medicine journals issued a statement in October 2020 pledging a commitment to DEI in order to combat the supposed evils of “systemic racism” in healthcare and medicine.
Here’s a brief excerpt:
“We will encourage and mentor authors from groups underrepresented in medicine. We will ensure that content includes an emphasis on cultural humility, diversity and inclusion, implicit bias, and the impact of racism on medicine and health. We will recruit editors and editorial board members from groups underrepresented in medicine.”
But, whereas many have since quietly removed their more explicit pledges to engage in political advocacy, DEI programming, or even overt racial discrimination, AFP’s are not only front and center but have been added to as recently as 2025.
Currently, AFP maintains a statement on the “Diversity” webpage advertising its work “developing goals to increase recruitment of authors, editors, and peer reviewers from underrepresented racial and ethnic groups.”
It’s unclear exactly how AFP aims to achieve this goal, but at first blush, this sure sounds like racial discrimination.
Also present on AFP’s Diversity webpage are a host of resources that evince the journal’s commitment to DEI and radical identity politics.
One resource, a 2022 editorial titled “Improving Diversity, Equity, and Inclusion in AFP,” includes admissions that the journal has actively tried to inject DEI into its content offerings.
“Regarding our editorial processes, we are increasing content on health disparities, racism, and social determinants of health; reevaluating the use of language regarding race, ethnicity, and gender; collecting anonymous demographic information from our authors after publication as we seek to improve representation and diversity; and encouraging mentorship of underrepresented minorities in medicine and medical writing,” the editorial states. “A dedicated editorial team meets regularly to discuss specific and general matters related to diversity, equity, and inclusion (DEI).”
Additionally, AFP appointed a “Medical Editor for Diversity, Equity, and Inclusion” in order to “support clinical content and curriculum”; the person appointed to this role, as of last year, appears to still hold that position.
It’s also worth noting that later this year, the AAFP is hostingan event titled the “National Conference of Constituency Leaders” which features representatives from several key “constituencies” of the organization.
These constituencies include “BIPOC physicians and those physicians who are supportive of and aligned with the issues faced by this group” and “Physicians who identify as LGBTQ+ and those physicians who are supportive of and aligned with the issues faced by this group.”
This appears to be yet another example of an approach to medicine more concerned with group identity than clinical excellence.
Do No Harm has frequently cataloged the AAFP’s infatuation with DEI; in 2024, we reported on AAFP’s efforts to recruit subject matter experts for its continuing medical education content, with proposals required to be “DEI-focused.”
And in 2023, the AAFP’s vice president of medical education bemoanedthe Supreme Court’s decision that found race-based university admissions unconstitutional, instead calling for alternative means of racial discrimination.
All in all, it seems like AAFP and its journal are still committed to pushing divisive, discriminatory, and radical ideology and practices.
Family physicians, and patients by extension, suffer as a result.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2602707605-1-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2026-01-15 19:51:572026-05-14 16:04:36American Family Physician’s DEI-Centric Restructuring
Boston Medical Center currently maintains on its website the “Glossary for Culture Transformation” (“the Glossary”), an exhaustive list of terms referring to various tenets of DEI ideology. Examples include “anti-racism,” “privilege,” “Latinx,” and many, many others.
As the Glossary webpage makes clear, these terms are intended to advance the DEI goals of Boston Medical Center, Boston University Medical Group, and related educational institutions.
Here’s how the Glossary webpage describes the creation of the Glossary:
“The Office of Equity, Vitality, and Inclusion, in partnership with Boston Medical Center, Boston University Medical Group, Boston University Chobanian & Avedisian School of Medicine, Boston University School of Public Health, Boston University Goldman School of Dental Medicine, and Boston University Graduate Medical Sciences collaboratively developed this Glossary as a tool to align our goals of justice, equity, and belonging and strengthen our collective understanding. Establishing shared language is foundational to creating common understanding by expanding our awareness of the world beyond our individual identities and experiences.”
So, in other words, all of these clinical institutions are culpable for injecting radical identity politics into healthcare through the Glossary.
The definitions of these terms are further evidence of this ideological goal.
For instance, the definition of “anti-racism” is sourced explicitly from Ibram X. Kendi, a radical proponent of racial discrimination on the basis of remediating past injustices.
“The only remedy to past discrimination is present discrimination,” Kendi has said. “The only remedy to present discrimination is future discrimination.”
It’s also worth noting that as recently as January 2025, Kendimaintaineda research center at Boston University.
The definition of “privilege,” meanwhile, falsely states that “White people in America are privileged in that their race will not limit their economic or educational prospects.”
Yet, Do No Harm has documentedcountless instances of medical schools explicitly excluding white and/or Asian students from educational opportunities on the basis of race.
And in medical school admissions, white and Asian students often facemuch longer odds of admission than their black and Hispanic counterparts with equivalent GPAs and MCAT scores.
Indeed, the Glossary contains several terms that appear laudatory of efforts to engage in racial discrimination.
The definition of “racial justice” reads as follows: “The creation and proactive reinforcement of policies, practices, attitudes, and actions that produce equitable power, access, opportunities, treatment and outcomes for all people, regardless of race.”
It should go without saying that any attempt to equalize “outcomes” among racial groups will invariably involve favoring some racial groups over others. Many such discriminatory policies are evenjustified under the guise of health equity or similar concepts.
Other entries are more overtly political.
The entry for “decolonization” includes a definition of decolonization as “the active resistance against colonial powers, and a shifting of power towards political, economic, educational, cultural, psychic independence and power that originate from a colonized nation’s own indigenous culture. This process occurs politically and also applies to personal and societal psychic, cultural, political, agricultural, and educational deconstruction of colonial oppression.”
What this has to do with Boston Medical Center’s (ostensible) goal of providing the best possible medical care is anyone’s guess. It seems instead to be evidence that Boston Medical Center is content to serve as a vehicle for radical political activism, at the expense of a focus on clinical excellence.
What’s more, as the Glossary’s webpage states, “the Glossary for Culture Transformation is a living document to be revised on an annual basis.”
If that is indeed true, then Boston Medical Center has been doubling down on its commitment to radical ideology.
Hopefully, it will rediscover fundamental principles of medical ethics – to strive to “do no harm” and provide the best possible care – and ditch identity politics for good.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1845309475-scaled.jpg14402560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2026-01-14 19:34:582026-05-14 16:04:59Boston Medical Center Maintains ‘Glossary’ Chock Full of Radical Ideology
Editor’s note: Do No Harm is a membership organization representing healthcare professionals, students, patients, policymakers, and concerned citizens of all faith backgrounds. We were invited to provide our medical expertise to assist leaders of a faith community in crafting guidance to address the challenges of gender ideology. Do No Harm’s contributions to this report are intended to provide the best possible medical and scientific information.
SALT LAKE CITY, UT;January 14, 2025 – This week, Do No Harm released a guide co-authored with the Coalition for Jewish Valuesentitled Rethinking Gender Affirmation. The guide is designed to properly inform observant Jewish parents on the challenging issue of gender dysphoria and expose progressive Jewish organizations injecting radical gender ideology into their teachings. The guide unites Jewish scriptures and sound science to debunk and reject so-called “gender-affirming care” on minors.
Organized in three key parts, the guide addresses the distress parents of gender-confused children face and provides answers to the influx of misinformation on the topic of gender dysphoria.
Part I: Sex and Gender in Jewish Law, clarifies in detail what the Jewish scriptures have to say on the topic of gender.
Part II: What the Science Says, addresses and debunks several popular scientific myths surrounding transgenderism and provides an overview of the lack of evidence supporting pediatric gender medicine.
Part III: Problems and Solutions, explains how education plays a key role in the transmission of values from one Jewish generation to the next and identifies the actors who continue to inject gender ideology into Jewish communities.
“Jewish parents of gender distressed minors have had nowhere to turn for scientifically sound and doctrinally-based guidance when navigating their child’s gender confusion,” saidIan Kingsbury, Director of Do No Harm’s Center for Accountability in Medicine. “Our first-of-its kind guide offers an alternative to the deluge of misinformation parents are fed by radicalized medical professionals pushing a pro-transgender agenda. The guide uses both medicine and Jewish scripture to strip the activists’ narrative and expose the lies of the radical gender cult.”
“We are delighted to collaborate with Do No Harm to bring this resource to the public,” said Rabbi Moshe B. Parnes, Southern Regional Vice President of the Coalition for Jewish Values. “In an environment where activists erroneously claim that Judaism recognizes ‘a wide range of gender identities,’ it is important for rabbis and laypeople to be equipped with the facts: that male and female are Divine creations, that these are unaffected by psychological difficulties, and that there are groups attempting to cloud these eternal truths in the vulnerable minds of our precious next generation. This is an important document that we hope will be studied broadly.”
Click here to read the report by Do No Harm and the Coalition for Jewish Values.
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. It has over 50,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 14 countries.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2026-01-14 16:20:172026-02-11 15:34:19Do No Harm Co-Authors Guide for Jewish Parents on Dangers of So-Called ‘Gender-Affirming Care’
Today, Do No Harm and Alliance Defending Freedom hosted a rallyon the steps of the Supreme Court as justices heard oral arguments in two cases, Little v. Hecox and West Virginia v. B.P.J, that concern Idaho and West Virginia laws restricting participation in girls’ and women’s sports to the female sex.
The cases have enormous implications not just for girls’ and women’s sports, but for truth, fairness, and the extent to which unscientific and ideological conceptions about sex can influence education and athletics. These laws recognize the reality of biological sex and protect girls from the harms of gender ideology.
The rally achieved a massive turnout, and featured a number of prominent speakers such as House Speaker Mike Johnson, Congressman Byron Donalds, and athlete and advocate Riley Gaines, as well as Do No Harm’s Chloe Cole, Dr. Travis Morrell, and Dr. Steve Ward.
https://twitter.com/i/status/2011154881260695803
Secretary of Education Linda McMahon, who praised the work of Do No Harm in her remarks, sounded the alarm over the rise of gender ideology in schools across the country.
“Gender ideology has transformed once great academic and athletic institutions into embarrassments, with tragic consequences for our women and for our girls,” she said.
“They reflect a real, troubling pattern of harm inflicted by radical forces looking to reshape our culture,” she continued.
Do No Harm Patient Advocate Chloe Cole shared her story of being subjected to dangerous sex-denying medical procedures as a child under the guise of gender ideology. She explained how the Supreme Court’s decision could open the door to further intrusion of gender ideology into education, healthcare, and elsewhere.
“[The Court is] being asked to rule on something that is even more fundamental: basic biological reality between the two sexes,” she said. “These nine justices are all that stands in the gap.”
“When biological reality is forsaken, it not only allows harm towards vulnerable children, but collateral damage to the rights of a whole sex,” she continued, characterizing gender medicine as “a complete lie.”
“If the biggest court in the land can defend the duty to protect children, then it must also protect all girls, and all women: our privacy, our safety, and our sports,” she concluded, referencing the Court’s decision in United States v. Skrmettiand urging the Court to “choose science, choose truth.”
Figure 1. Dr. Travis Morrell speaks on the steps of the Supreme Court.Figure 2. Dr. Steve Ward speaks on the steps of the Supreme Court.
You can watch full coverage of Do No Harm and ADF’s rally here.
Inside the courthouse, much of the arguments – and questions from the justices – centered on the biological differences between girls and boys that serve as the basis for the Idaho and West Virginia laws.
Associate Justice Samuel Alito posed questions that got to the heart of the case: the reality of biological sex.
“For Equal Protection purposes, what does it mean to be a boy or a girl, or a man or a woman?” Alito asked attorney Kathleen Hartnett, representing the plaintiff in Little v. Hecox.
However, Hartnett failed to provide a definition.
Alito also stressed the fundamental physical differences between male athletes and female athletes in questions to the plaintiffs’ attorneys.
“What do you say about them? Are they bigots?” Alito asked. “Are they deluded in thinking they are subjected to unfair competition?”
In sum, the outcome of these cases will have enormous consequences not just for girls’ and women’s sports, but will be a referendum on truth, fairness, and basic common sense.
As Do No Harm explained in our amicus brief, sex is real and binary.
Do No Harm urges the Supreme Court to recognize biological reality and decide these cases accordingly.
https://donoharmmedicine.org/wp-content/uploads/DNHRally1.jpeg15362048Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2026-01-13 20:14:542026-06-05 13:56:18Do No Harm and Alliance Defending Freedom Host Rally on Supreme Court Steps
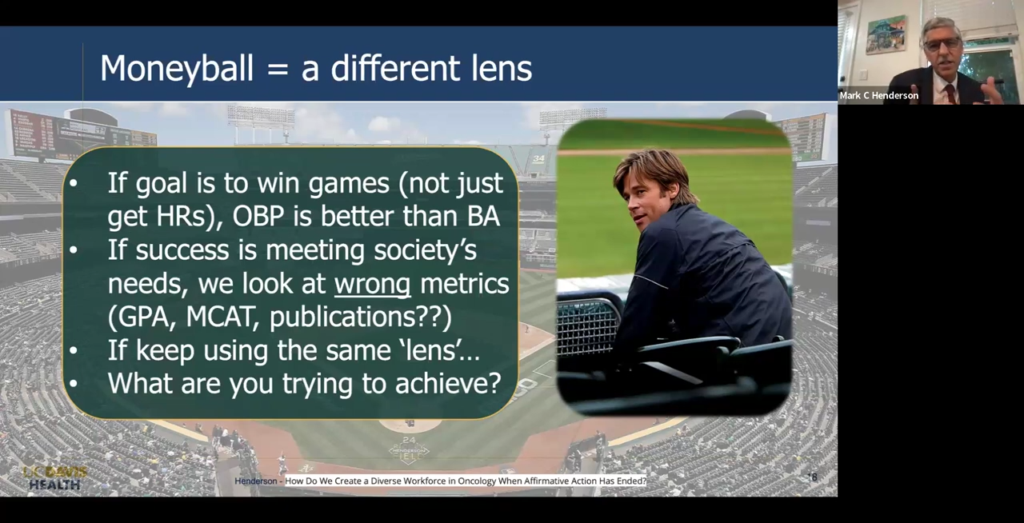
“If success means meeting society’s needs, we’re probably looking at the wrong measures at this point […]: grade point average, MCAT, publications. There’s not a lot of evidence that those measures actually improve health outcomes in society.”
Those are the words of Mark Henderson, MD, the Associate Dean for Admissions at the University of California, Davis School of Medicine. Henderson made the comments at an October 2024 grand rounds session hosted by Stanford Medicine’s Obstetrics and Gynecology department titled “Cultivating Physicians Our Nation Needs After Affirmative Action Ended.”
There, Henderson discussed ways that medical schools and graduate medical education programs could continue to engage in diversity initiatives and discriminatory practices in the wake of the Supreme Court’s decision in Students for Fair Admissions v. Harvard, which found race-conscious admissions to be unconstitutional.
A key point: Henderson’s comments are particularly noteworthy as California has banned race-conscious admissionsfor decades, and yet UC Davis has succeeded in diversifying its student body through its “socially accountable”admissions practices(more on that later).
One doesn’t need to read between the lines of Henderson’s comments: he is explicitly calling for schools to devalue objective metrics of academic achievement like GPA and MCAT scores in favor of criteria that favor qualities such as diversity. As Henderson later says, the mission of UC Davis Medical School is to “matriculate future physicians who will address the diverse health workforce needs of our region.”
Of course, Henderson’s premise is just not true; MCAT scores, for example, are predictive of performance on Step 1 and Step 2 of the U.S. Medical Licensing Exam or USMLE, which is in turn predictive of clinical performance.
Figure 1. A slide comparing UC Davis’ admissions strategy to “Moneyball.”
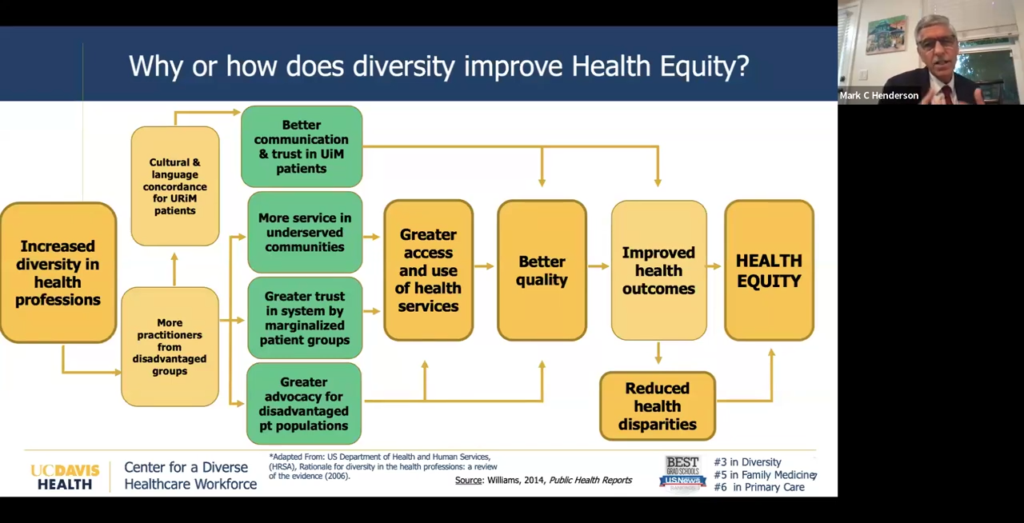
To justify this DEI-centric approach to admissions, Henderson makes the argument that a diverse healthcare workforce actually leads to better health outcomes for patients.
Figure 2. A slide touting the supposed benefits of diversity in the healthcare workforce.
Henderson, without explicitly using the words “racial concordance,” alludes to the notion that patients (particularly patients belonging to racial minorities) will experience better health outcomes when treated by physicians of the same race.
As Do No Harm has repeatedly shown, this argument, commonly employed to justify discriminatory diversity hiring practices in healthcare, isbunk. Five out of six systematic reviews find that racial concordance has no impact on health outcomes.
That hasn’t stopped Henderson and co., of course. Indeed, UC Davis tied for the lowest marks in the Center for Accountability in Medicine’s Medical School Excellence Index, which assesses medical schools on their commitment to academic achievement and merit over radical ideology.
To achieve its diversity goals, Henderson touted UC Davis’s “socially accountable” admissions strategy, which aims to deemphasize measures of academic achievement in favor of measures that appear to be proxies for diversity.
This behavior isn’t new from Henderson and UC Davis: Do No Harm previously reported on a 2022 webinar in which Henderson, discussing UC Davis’s admissions process, stated that the “overrepresentation” of Asian physicians is addressed through an “institutional diversity and inclusion policy that explicitly and publicly states our priorities for recruitment based on the statistical gap between California’s population and the physician workforce demographic of underrepresented groups.”
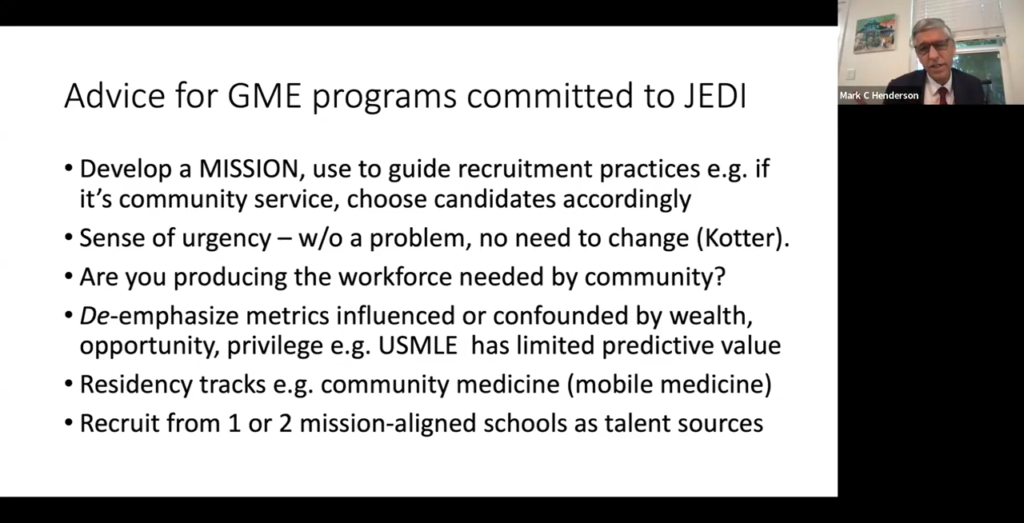
Next, Henderson took care to stress that the Supreme Court’s decision did not apply to graduate medical programs, such as residency programs, and encouraged them to continue to engage in diversity initiatives consistent with local laws and federal civil rights law.
Again, Henderson encouraged programs to de-emphasize metrics of academic achievement, which Henderson characterized as being “confounded” by wealth and “privilege.”
Figure 3, A slide discussing legal advice for graduate medical education programs.
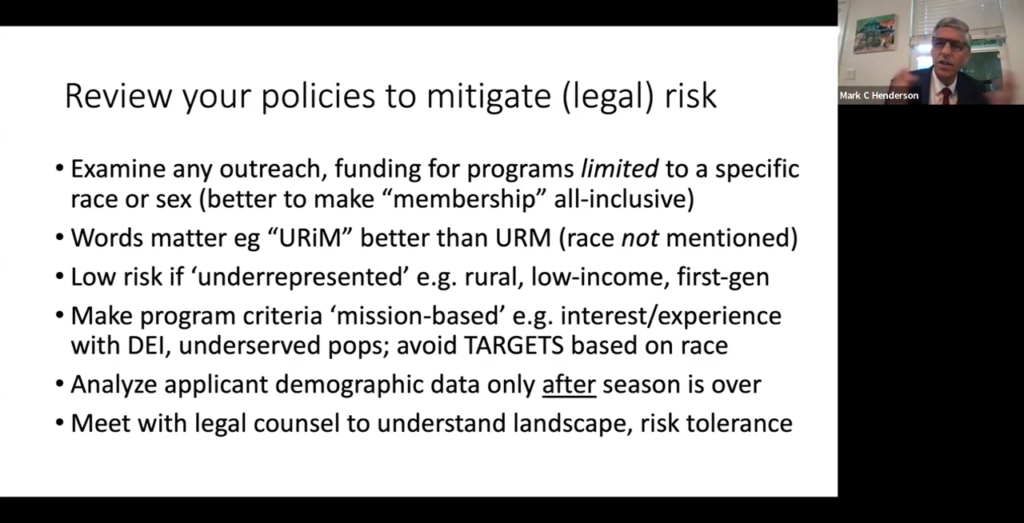
Next, Henderson offered ways for programs to mitigate their legal risk by cloaking DEI initiatives in terms that may obscure their racial focus.
“Words matter. ‘Underrepresented in medicine’ is a term that means that the population, whatever the identity is, is underrepresented relative to the population,” Henderson said. “That’s better than ‘underrepresented minority,’ which refers to racial identity.”
Figure 4. A slide discussing ways for GME programs to mitigate their legal risk.
And finally, Henderson concluded by encouraging residency program directors to balance the legal risk of discriminatory practices and policies with the goals of diversity.
“Try to light some fires,” he said, urging residency programs to follow their (DEI-centric) missions.
Well, there is one surefire way to mitigate risk: stop engaging in discriminatory diversity initiatives that treat individuals on the basis of their race, rather than their merit.
Unfortunately, this seems to be a bridge too far for Henderson and UC Davis.
https://donoharmmedicine.org/wp-content/uploads/2022/12/image-9.png3481475Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2026-01-13 13:23:022026-02-11 15:34:18UC Davis Admissions Dean Discusses Ways to Continue DEI Despite Legal Obstacles
This week, the American Board of Internal Medicine (ABIM), which certifies physicians in the field of internal medicine, sent out anupdate to its members summarizing the fall meeting of its Infectious Disease Board.
But that update, among other things, also contained a statement doubling down on ABIM’s DEI practices.
“ABIM continues to work in the areas outlined in the Equity Statement: developing health equity content for assessments, ensuring that assessments are fair, and researching to advance assessment strategies,” the update continues. “ABIM also maintains collaborations with medical specialty societies working to advance health equity. During this session, staff highlighted both the progress achieved and the challenges that remain in ABIM’s ongoing health equity efforts.”
The Health Equity Statement makes clear that ABIM is injecting “health equity” into the certification process: “We include health equity content in our assessments, based on science and evidence related to health disparities.”
It’s unclear exactly what this means: Health equity is a nebulous term, but often refersto practices that seek to equalize health outcomes between racial groups, often through racial discrimination.
Moreover, the premise for these practices is that racial disparities in health outcomes are explained by systemic racism or some other factor that is best addressed through political/social change.
Regardless of the exact manner in which ABIM is infusing “health equity” into its assessments, that these topics are included in the certification process is cause for alarm.
But that’s not all.
Indeed, ABIM maintainsa webpage dedicated to its commitment to health equity, replete with various DEI resources and evidence of the organization’s DEI activities.
“Like many organizations across the United States, the American Board of Internal Medicine (ABIM) and ABIM Foundation (ABIMF) are at a turning point, where we move from being ‘passively non-racist’ institutions to committing ourselves to be an ‘actively anti-racist’ influence in health care,” that webpage reads.
Anti-racism, defined by its most prominent proponent Ibram X. Kendi, refers to a set of practices that explicitly seek to remedy past discrimination through present racial discrimination.
Internally, ABIM appears to be adhering to these principles. For instance, it describes itsvarious committeesand councils as aiming “to maintain a composition that reflects the diversity and complexity of the physician and patient populations that certification serves.”
ABIM’s 2020 statement on racial justice also includesa pledge to engage political activism: “we pledge actively to do our part in opposing and dismantling systems and policies that cause harm to our patients and disproportionately affect those in Black and Brown communities.”
“Develop and implement programs that address the racial and ethnic disparities in health care”;
“Influence the education and training of board certified internists to equip them with the skills and awareness to recognize and prevent healthcare disparities and to promote health equity”; and
“Intentionally create and foster partnerships to exponentially expand the impact of ABIM’s efforts in addressing systemic racism and disparities in health care, in the healthcare profession, in the provision of health care and the outcomes of that care.”
As an organization that certifies physicians, ABIM’s chief concern should be the competency of medical practitioners.
Instead, it seems that ABIM has decided that “health equity” and other DEI concerns should be its focus.
And, as the recent update demonstrates, ABIM is doubling down.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2267532547-1-scaled.jpg17082560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2026-01-09 17:33:512026-05-14 16:06:35American Board of Internal Medicine Doubles Down on DEI
Like many medical schools over the past several years, the Kaiser Permanente Bernard J. Tyson School of Medicine (Kaiser) has undergone a bit of a facelift.
Yet the actual content of the current webpage still makes clear that Kaiser is committed to DEI, with the maxim “Diversity Unites Us” front and center.
“We believe diversity brings us together. It inspires us to respect the experiences and perspectives of others,” the page reads. “Diversity encompasses much more than culture, race, and religion.”
Nevertheless, there have been some changes. For instance, a 2024 version of the webpage included the statement that “equity, inclusion, and diversity are woven into every aspect of Kaiser Permanente Bernard J. Tyson School of Medicine, including pipeline efforts, admissions, staffing, curriculum, student support, and community.”
It’s hard to see how the pursuit of racial diversity could be “woven into” admissions and staffing efforts in a way that would not be discriminatory: any effort to increase the number of students from certain racial groups invariably comes at the expense of other racial groups.
Additionally, resources that cataloged DEI activities at Kaiser are no longer present.
These include an overviewof Kaiser’s DEI commitments that includes explicit admissions of racial discrimination.
Here are few highlights:
“[Kaiser] has embedded anti-racism and related topics throughout its curriculum…”
“Our commitment to diversity is illustrated in the composition of our student body, which is among the most diverse in the country.”
“Our approach to student admissions is to evaluate the full experience of each individual, including academic, personal, and other characteristics that contribute to defining the whole person. This approach increases the likelihood of admitting students from diverse backgrounds.”
“For all recruitment of board members, administrators, faculty, and staff, whether by search firms, human resources professionals, or faculty committees, the school has been intentional in its goal to hire and appoint individuals from a diversity of backgrounds and experiences.”
And there are many, many more examples.
Another resourceno longer present on the Office of Inclusive Excellence’s webpage is the school’s 2021 “Anti-Racism and Equity, Inclusion, and Diversity Plan.”
That plan included activities that the school had taken such as:
“Development of an anti-racism curriculum for students.”
“Intentional and equitable board, leadership team, faculty, and staff recruitment.”
“Universal equity, inclusion, and diversity training for faculty, staff, and students.”
Although these resources have since been removed from the school’s website, evidence of racially discriminatory behavior remains.
Indeed, Kaiser’s webpage on its admissions requirements outright says that the school uses a “holistic review” process for the purposes of pursuing diversity.
“However, know that your test scores and coursework will be reviewed in the context of your experiences, milestones, and personal attributes,” the webpage reads. “We believe this holistic review process will not only help us form a multidimensional portrait of each applicant, but also recruit and admit a diverse, inclusive, and highly qualified class.”
Moreover, according to 2024 admissions data reviewedby Do No Harm, Kaiser actually experienced an increase in the number of black and Hispanic matriculants following the Supreme Court’s decision holding that race-conscious admissions were unconstitutional. This is contrary to what one would assume following the implementation of a color-blind admissions regime. This is because black and Hispanic applicants had, on average, lower MCAT scores than their Asian and white counterparts, so one would expect their share of Kaiser’s matriculating students to decrease.
As Do No Harm’s “Skirting SCOTUS” report notes, this “casts serious doubt about adherence to the Court’s ruling against affirmative action.”
So, how should we examine these facts? On one hand, Kaiser has deleted much of the more egregious public-facing examples of its DEI commitments. But on the other hand, many DEI references remain.
And there is data suggesting that, well after the Supreme Court’s ruling, the school is still engaging in race-conscious admissions.
Taken together, all of this evidence suggests that Kaiser is removing only the most egregious and obnoxious references to DEI ideology while deep down, nothing has changed.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2111879009-1-scaled.jpg15462560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2026-01-09 15:41:032026-05-14 16:06:15DEI By Any Other Name? Kaiser Med School’s Rebrand Leaves ‘Diversity’ Commitments Intact
https://donoharmmedicine.org/wp-content/uploads/iStock-1401401407-1.jpg14102126dnhprodhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngdnhprod2026-01-08 20:15:252026-02-11 15:34:18Do No Harm’s DEI Tracker Flags 36% of U.S. Medical Schools
These sessions, which fulfill the Michigan Department of Licensing and Regulatory Affairs (LARA) “implicit bias training requirement,” have little to do with improving patient care and everything to do with advancing a particular ideological agenda.
The first red flag appears immediately in the module “DEI: Past, Present and Future.”
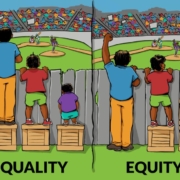
The module begins by comparing DEI to a “party”: diversity is being invited to a party, inclusion is being asked to dance, and equity is “leveling the playing field” and “dancing without barriers.” Accompanying this is the misleading illustration of children on boxes watching a baseball game.
But here’s what’s missing: in practice, “equity” here means discriminating based on race and other immutable characteristics to achieve predetermined outcomes. The Civil Rights Act of 1964 explicitly prohibits such discrimination, a fact the training materials themselves acknowledge when citing the Act and Executive Orders 10925and 11246.
The irony is apparently lost on the presenters.
Later in the presentation, we encounter this little tidbit: race has become “ambiguous” because it’s now about one’s internal self-identification and has lost any degree of objectivity.
Let’s think this through. If race is whatever someone identifies as, then why can’t anyone identify as anything that advantages them? And if they can, doesn’t that render the entire DEI framework meaningless?
One can’t simultaneously claim that racial categories are socially constructed fictions and use them as the basis for medical policy and resource allocation.
The training also includes “The Gardener’s Tale” video, adapted from Dr. Camara Jones, meant to illustrate “institutional racism” via the analogy of a gardener who prefers red flowers over pink, and therefore grows the red flowers in more fertile soil.
It patronizes black Americans by suggesting they cannot succeed without external intervention to overcome systemic barriers – barriers that, conveniently, only the DEI apparatus can identify and remedy.
This paternalistic approach is deeply condescending. It treats minority patients not as autonomous adults capable of navigating the healthcare system, but as victims requiring constant accommodation.
Scholars such as John McWhorter have pointed out that this methodology treats concepts like systemic racism more like a religion than a working theory about society, and in so doing, ignores the multitude of factors – such as personal choice, biological factors, and medical comorbidities – that lead to disparities.
Understanding the true causes of outcome disparities, for example, matters in the context of healthcare and requires moving past the simplistic assumption that all difference is the product of “systemic racism.”
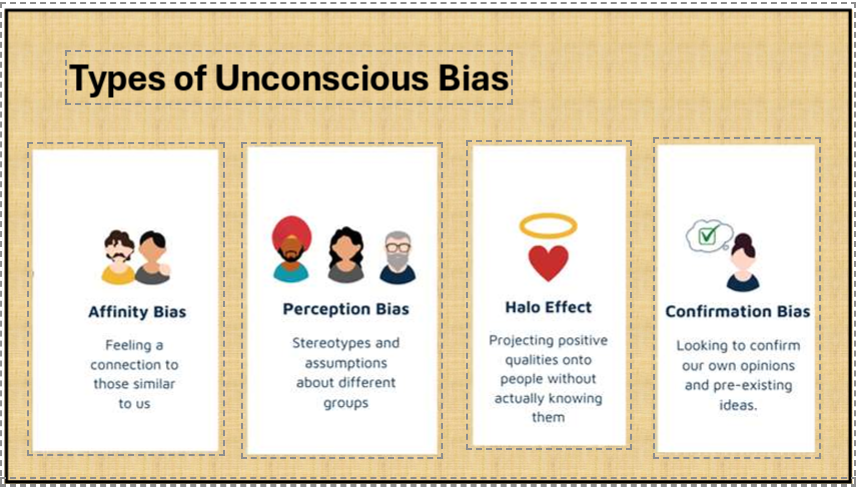
Additionally, the module on “Implicit Bias and its Impact on Health Equity” lists several types of unconscious bias: affinity bias, perception bias, the halo effect, and confirmation bias.
Figure 2. From “Implicit Bias and its Impact on Health Equity.”
When discussing implicit bias, the training cites the Implicit Association Test (IAT) as evidence of bias.
Figure 3. From “Implicit Bias and its Impact on Health Equity.”
However, the IAT has been thoroughlydebunked as a predictor of discriminatory behavior. Even its creators have backed away from strong claims about its validity. Yet here it is, presented uncritically as scientific fact in physician training.
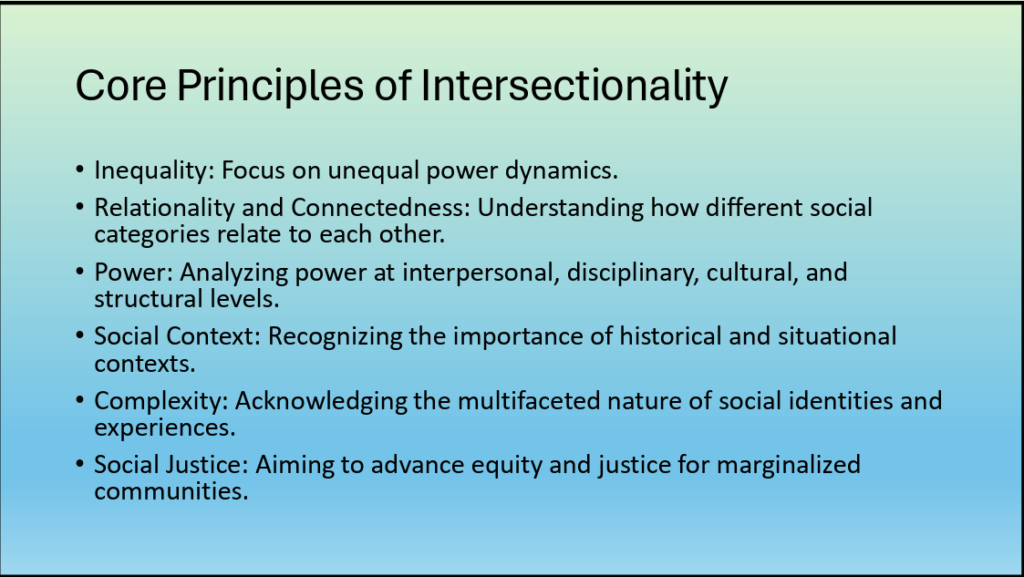
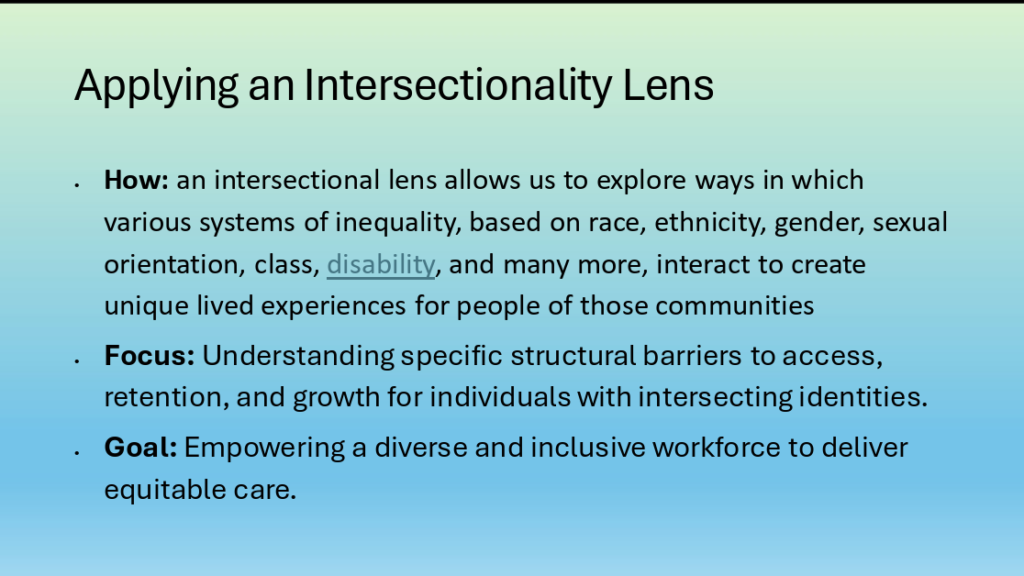
The module “Beyond Equity, Diversity, and Inclusion: The Power of Intersectionality in Addressing Bias” takes things even further. Slide after slide smuggles in radical ideology under the guise of healthcare improvement.
“Intersectionality” – a framework borrowed from critical theory that is used to combine different categories of how one identifies, such as being a certain race, religion, and sexuality – is presented as an established fact.
Figure 4. From “Beyond Equity, Diversity, and Inclusion: The Power of Intersectionality in Addressing Bias.”Figure 5. From “Beyond Equity, Diversity, and Inclusion: The Power of Intersectionality in Addressing Bias.”
These ideas explicitly advance a vision of healthcare that treats individuals in accordance with their group identity, and one in which the pursuit of social justice is central to shaping care within that framework.
So much for doctors focusing on their trade of providing good, quality medical care; now they’re called to be social justice warriors.
What is particularly concerning is that these training sessions represent thousands of hours of physician time and mental energy diverted from actual medical education and patient care. Instead of learning about the latest clinical evidence or honing diagnostic skills, Michigan physicians are subjected to ideological indoctrination that treats them as presumptively bigoted and in need of political re-education.
The presentations, taken as a whole, indicate a clear desire to radicalize participants rather than educate them. For example, it treats any attempt to restrict these divisive DEI programs as a sort of bogeyman; as if it would be disastrous to curb their efforts, but no evidence is given to back up this notion.
Figure 6. From “Beyond Equity, Diversity, and Inclusion: The Power of Intersectionality in Addressing Bias.”
At one point, the materials state: “Health professionals must increase their awareness of anti-DEI misinformation and propaganda, and communicate clearly about the tremendous value of diversity, equity, inclusion, and antiracism.”
Figure 7. From “Beyond Equity, Diversity, and Inclusion: The Power of Intersectionality in Addressing Bias.”
Translation: anything opposed to the standard line about DEI is misinformation and propaganda, and healthcare professionals should not entertain the possibility of another theory.
Is that how medical science is advanced – through dismissing competing ideas as misinformation?
The Michigan State Medical Society should ask itself a simple question: Are Michigan patients receiving better healthcare because their physicians attended these training sessions? That’s doubtful, particularly given the lack of supporting evidence.
What’s clear is this: Medical care should be based on clinical evidence, individual patient needs, and the physician’s judgment – not on contested theories about social construction, intersectionality, and systemic oppression. Our patients – all of them – deserve better.
https://donoharmmedicine.org/wp-content/uploads/equality-equity.jpg627851Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2026-01-08 18:03:042026-02-11 15:34:18Michigan State Medical Society’s DEI Training: Ideology Masquerading as Medicine
The Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN) has the ostensible missionto “support nurses caring for women, newborns, and their families.”
However, several of the organization’s position statements reveal another agenda: advocating for injecting radical identity politics into healthcare.
AWHONN’s position statementon “Racism and Bias in Maternity Care Settings,” citing several examples of racial disparities in health outcomes, asserts that the role of nurse should include advocacy to confront supposed systemic racism in healthcare.
“Nurses must seek to change the structures, institutions, attitudes, beliefs, and practices that have legally or otherwise perpetuated racism, discrimination, mistreatment, and lack of treatment of Black women in the U.S. healthcare system,” the statement reads.
One such way nurses can do this, the position statement suggests, is through confronting “implicit bias.” Keep in mind that “implicit bias” is a poor predictor at best of any real-world health outcomes.
Nevertheless, AWHONN maintains that it will work to “[e]ncourage all states and territories to develop legislation such as the California Dignity in Pregnancy and Childbirth Act(2019), which requires perinatal health providers and staff to receive training on implicit bias.”
Other policy recommendations are to:
“Encourage states and health care organizations to provide funding for nurses to receive anti-racism, bias, and cultural competency education during clinical training and practice”;
“Expand equitable access to models of care that provide the most optimal outcomes, such as community-based programs, full spectrum doulas, and midwifery care”; and
“Expand funding to support research efforts to examine the role and impact of racial bias.”
Most disturbing, however, is the statement that AWHONN will “[s]upport programs and initiatives to diversify the current nursing and health care workforce.”
It’s unclear how, exactly, AWHONN aims to achieve this without calling for explicitly discriminatory hiring and recruiting practices.
But we don’t have to speculate.
AWHONN’s “Nursing Workforce Diversity” position statement is rife with explicit commitments to engage in these discriminatory practices.
Here are just a few recommendations that make clear how AWHONN is committed to DEI:
Ensure that recruitment and educational materials represent a diverse nursing workforce.
Implement holistic admission review policies by academic institutions.
Provide equitable clinical opportunities for students based on course and program outcomes.
Identify barriers that hinder admission for and successful graduation of underrepresented students.
Expand tuition assistance and other financial agreements for underrepresented students.
Increase recruitment of diverse nursing faculty and academic leaders.
Recruit, hire, and support a diverse workforce of nurses that represents the communities they serve.
Provide training and educational resources that support and represent workforce diversity.
Several of these recommendations are worth expanding on.
“Holistic review” refers to admissions practices that devalue metrics of academic achievement in favor of “softer” factors such as personal traits. That AWHONN believes implementing this process will increase diversity is extremely telling, as it’s suggesting that holistic review is really a proxy for racial discrimination. And for what it’s worth, in the medical school context, we have strong evidence that it is.
Providing “equitable clinical opportunities” would appear to entail some form of discriminatory system that allocates opportunities to acquire clinical experience on the basis of race. This is, admittedly, speculative, but does seem par for the course when viewed in conjunction with the other recommendations.
All told, it’s clear that AWHONN is intent not only on serving as a vehicle for DEI activism in healthcare, but also as an engine of discrimination in nursing.
Racial discrimination has no place in healthcare: not only is it unethical and unfair, but it degrades the quality of the healthcare workforce by prioritizing identity over merit.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2213352297-scaled.jpg17082560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2026-01-06 18:55:372026-05-14 16:07:14Major Nursing Org Embraces Racial Discrimination and DEI Activism
“Diversity, equity, and inclusion are not just buzzwords. They represent an essential element of our society.”
That’s what Dr. Joaquin Sanchez-Sotelo, then-president of the American Shoulder and Elbow Surgeons (ASES), said in a January 2025 videopromoting the organization’s DEI committee and various diversity efforts.
The video specifically highlighted the ASES’s various DEI initiatives and attempts to boost diversity in this orthopedic subspecialty.
For instance, one of the co-chairs of the ASES’s DEI committee, Dr. Sara Edwards, discussed the partnerships and programs the ASES engages in to further these goals.
“[W]e also give several scholarships to our residency programs […] and get [residents] exposed to shoulder, elbow again in an attempt to recruit more diversity within our field,” Dr. Edwards said.
Both Dr. Edwards and Dr. Sanchez-Sotelo discussed ASES’s partnership with nonprofit organization Nth Dimensions.
According to an archived versionof Nth Dimensions’ “About” webpage, Nth Dimensions’ mission was to create a talent pipeline “to address the dearth of women and underrepresented minorities (URMs) in orthopaedic surgery.”
However, that language has since been removed from the organization’s website.
Additionally, the “Become an Nth Scholar” webpage previously advertised the organization’s “ongoing mission to diversify the physician workforce.”
Indeed, in the ASES January 2025 newsletter, the organization characterized Nth Dimensions’ summer internship program as helping “build professional relationships as well as mentorship opportunities for under-represented minorities while giving these young medical students the chance to learn more about Shoulder and Elbow surgery.”
The ASES newsletter also hints at several other initiatives that suggest potentially discriminatory recruiting patterns: “There are a number of DEI achievements we can celebrate […]: advisory role when faculty is selected for various programs, selection of scholars for the Nth Dimensions summer internship, funding support for underserved individuals that wish to attend the ASES Fellows and Residents Course, and further collaboration with Nth Dimensions and other organizations to bring high school, college and medical students to our Annual Meeting and expose them to what ASES has to offer.”
Taken together, it’s clear that the ASES is hyper-fixated on increasing diversity within this orthopedic surgery subspecialty and engaging in potentially discriminatory practices to achieve this goal.
This undermines the very foundation of medicine, which should prioritize competence, training, and skill above all else.
Limiting opportunities based on group identity rather than individual merit is inherently discriminatory and contrary to basic principles of fairness and excellence in patient care.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2013632891-scaled.jpg13082560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2026-01-06 14:42:072026-05-14 16:07:31DEI Runs Wild Within the American Shoulder and Elbow Surgeons
The Georgetown University Hospital/Washington Hospital Center Emergency Medicine Residency Program appears intent on inserting DEI into its core educational activities.
“We understand that an inclusive academic program will enrich our learning environment and improve care of the patients we serve,” the program’s DEI page reads. “Our program is dedicated to recruiting and retaining a diverse group of residents and faculty.”
If that seems like just the usual jargon paying lip service to DEI, think again.
The program boasts a $1,500 diversity scholarshipintended to “[r]ecruit and retain a diverse residency class to best reflect the diverse population that our program serves.”
This appears to be a subtle, indirect gesture at the (debunked) notion that patients experience better health outcomes when treated by physicians of the same racial group.
The scholarship description also states that applicants will “ideally” have an “interest in diversity & inclusion in the equitable delivery of healthcare.”
While the scholarship criteria disclaim any overt racial discrimination in the application process, they do state that 4th-year medical students “from groups underrepresented in medicine” are especially encouraged to apply.
Next, DEI is incorporated into the program’s curriculum. The program’s diversity page states it best:
Diversity and inclusion permeates all aspects of our curriculum. Every clinical shift our residents have the opportunity to care for and learn from a profoundly diverse patient population. We offer elective rotations focused on the care of unique populations. During didactics, we address the importance of diversity and inclusion via lectures, journal clubs, workshops, small group discussions, and simulation. We highlight the importance of understanding and mitigating implicit bias.
Indeed, the curriculum contains a host of political and DEI-related sessions including “Advancing Health Equity in Emergency Medicine”; “Microaggressions in Clinical EM Simulation”; and “Implicit Bias Workshop for Residents.”
Additionally, much of the scholarly work listed on the program’s diversity webpage matches the political nature of the program’s curriculum, with ample references to DEI and related concepts.
In this case, we don’t need to read between the lines.
As the program’s diversity page states, “diversity and inclusion permeates all aspects” of the Georgetown University Hospital/Washington Hospital Center Emergency Medicine Residency Program’s curriculum.
Unfortunately, Georgetown’s program seems more concerned with indoctrination and ideology, and less concerned with training the next generation of emergency physicians to be as competent as they can.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1189798267-scaled.jpg14402560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-23 22:55:592026-05-14 14:43:36Georgetown’s Emergency Medicine Residency Program Makes DEI A ‘Top Priority’