In a spectacular turnaround, the Kentucky Board of Nursing (KBN) has quietly rescinded its prior requirements for all nurses in the state to take implicit bias training as a condition of licensure.
The deadline for completing an approved implicit bias course was July 1, 2023. However, according to the KBN website as of July 27, the mandate has been removed. “If you have not obtained the training at this time,” the Continuing Education Competency webpage states, “please note you will no longer be required to do so.”
Figure 1. KBN website as it currently appears.
Do No Harm was the first to report in September 2022 that the KBN was endorsing the course titled Implicit Bias in Healthcare by the Kentucky Nurses Association (KNA) at a cost of $5.00 per KNA member (the non-member price is $35.00 per course). But, as a result of our reporting, a Kentucky-based Do No Harm nurse member’s appeal to the American Nurses Association, and subsequent media attention to the inflammatory and discriminatory nature of the course, the KBN attempted to cover its tracks by scrubbing its website of the KNA recommendation.
Figure 2. Mandatory courses available from the Kentucky Nurses Association as of August 9, 2023.
While Do No Harm applauds the removal of the mandate, we still have some questions. The requirement for this training is outlined in the Kentucky Administrative Regulations. Where did the discussion take place about removing the mandate, and who made that decision? Who is going to refund the money that more than 100,000 RNs, LPNs, and advanced practice nurses with an active Kentucky license would have needed to spend on obtaining this training since June 2022? Where does the money go that is paid to the KNA for this course?
We are asking these questions and monitoring this situation as it evolves.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_732496792-scaled.jpg13012560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-08-09 19:52:202026-05-11 12:52:30The Kentucky Board of Nursing’s Backpedaling on Bias Training Comes Full Circle
Will medical schools stop discriminating by race? That’s the big question following the Supreme Court’s recent decision ending so-called “affirmative action” in college admissions. Most medical schools are trying to find workarounds, but one Texas institution appears to be doing the right thing.
We submitted FOIA requests to Sam Houston State University’s osteopathic college. We asked for all internal communications regarding the Supreme Court’s decision. Lo and behold, we received a document from the director of admissions:
“I wanted to update you on some changes we are implementing in our COM admissions system (AMP) in response to the recent Supreme Court ruling… We have contacted AMP to initiate the necessary updates to our system. The plan is to completely remove race and ethnicity from the system until after offers are sent. This will ensure that our COM admissions process fully complies with the ruling and that all applicants are evaluated without any potential bias.” (emphasis added)
Did you catch that? Sam Houston State University’s osteopathic college will be unable to make admission decisions based on applicants’ race. That means no overt racial discrimination. The school will learn about applicants’ race only after the admissions process ends (presumably to comply with deferral reporting requirements).
This is the bare minimum change that every medical school should immediately make. At the same time, medical schools should commit to avoiding other ways of trying to discover and admit applicants based on race. If medical schools won’t stop discriminating, they deserve to be held accountable in the court of law and public opinion.
For now, at least, we’re grateful that Sam Houston State University is showing the way forward.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_533282275-scaled.jpg16812560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-08-09 19:52:012026-05-11 12:56:41Good News: This Texas Osteopathic School Is Going Colorblind
In April 2023, we reported that the University of Kansas School of Medicine (KUSM) at the KU Medical Center (KUMC) removed the racially discriminatory eligibility criteria from the Urban Scholars program, which was described as a “hallowed program” by a Kansas state representative, who is also a primary care physician. But KUMC is again under investigation for the two scholarships we described in our April posting.
On July 13, Do No Harm senior fellow Mark Perry was informed of the new investigation by the U.S. Department of Education’s Office for Civil Rights (OCR). A subsequent review of the KUMC website showed that the school had already modified the webpage for the Summer Diversity Research Scholarship, and had taken down the page for the Sub-Internship in Plastic Surgery Diversity Scholarship.
At the time of the complaint, eligibility for the Summer Diversity Research Scholarship was limited to students who are “a member of a population that is underrepresented in Plastic Surgery: i.e., African American/Black, American Indian, Native Hawaiian, Alaska Native and/or Hispanic/Latino.”
Figure 1. KUMC Summer Diversity Research Scholarship for First- and Second-Year Medical Students page as seen on April 14, 2023 (archived page here).
Today, the scholarship is open to all first- or second-year medical students in good standing, and “students who are members of groups underrepresented in medicine are encouraged to apply.”
Figure 2. Current eligibility criteria for the KUMC Summer Diversity Research Scholarship for First- and Second-Year Medical Students.
The Sub-Internship in Plastic Surgery Diversity Scholarship had the same discriminatory and illegal eligibility criteria.
Figure 3. KUCM Sub-Internship in Plastic Surgery Diversity Scholarship as seen on April 14, 2023.
However, instead of opening that scholarship to all eligible U.S. medical students, the Department of Plastic Surgery scrubbed the program from its website.
Figure 4. Current appearance of the webpage for the Sub-Internship in Plastic Surgery Diversity Scholarship.
Do No Harm applauds this outcome and will continue to pursue civil rights complaints against medical schools like KUMC that violate federal law.
Have you seen discriminatory scholarships or fellowships at your college or university? Please let us know; you may remain anonymous if you wish.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1442496242-scaled.jpg17092560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-08-08 11:25:442026-05-11 13:02:46The University of Kansas Continues Its Clean-Up Efforts in Response to a Second Federal Civil Rights Investigation
When members of Do No Harm attended the 2023 Endocrine Society meeting, we heard from many endocrinologists who quietly expressed concerns about current standards of care in pediatric gender medicine. A recent post on the anonymous social media platform Reddit reveals that those sentiments are not unique to one specialty.
A post in the medicine Subreddit (i.e., a section of the site devoted to medical discussion) raises serious technical concerns about a New England Journal of Medicine paper used to justify medical transition of children. While the critique is astute, it is not new. The paper rightfully caught tremendous flak for concluding that medical transition is beneficial for children. Among the red flags: the study featured no comparison group, so it’s impossible to discern how changes in mental health associated with transition compared to alternative approaches. Moreover, self-reported measures of mental health barely changed once children initiated hormonal intervention, and in fact were entirely static in natal males and those who initiated puberty blockers early in puberty. The individual who posted the critique mentions these reasons among their “serious concerns about pediatric gender medicine outcomes.”
If groups like the Endocrine Society and American Academy of Pediatrics were correct that their positions are backed by consensus, then one would expect the responses to rebuke the original post as fringe opinion. Instead, the commentators nearly universally express the same concerns. Among highly upvoted comments:
“I’m also a psychiatrist (although not CAP) [child and adolescent psychiatrist] and I agree there are significant limitations in the current evidence base supporting medical interventions for gender dysphoria, especially in minors… Often times, when this is brought up, the knee-jerk response is ‘but WPATH guidelines are the standard of care.’ Except WPATH guidelines are not grounded in robust evidence. And those who follow the organization know the changes that have happened in recent years. Former leaders being ousted because they’ve called for moderation and not jumping into blind affirmation without the evidence base to support that approach. The organization is not a neutral, professional scientific body and that major fact is often glossed over… To be blunt, psychiatry has a checkered history of too hastily adopting novel treatments without adequate study. Compassion for gender dysphoric individuals is important. Recommending irreversible medical interventions in vulnerable populations should require definitive, or at the very least probabilistic, proof of long-term benefit and minimal harm. Currently, that proof does not exist.”
“Internist, not psychiatrist. It’s bizarre to me that this is the only condition where we take at face value that what the patient says is wrong with them is exactly what’s wrong with them. Maybe you were born in the wrong body. Or maybe you’re a teenager which means that you’re going to try on multiple identities over the course of your adolescence before you find the real one. Or maybe you have borderline personality disorder and so have an unstable sense of self and are clinging to the current socially acceptable fix for a pervasive sense of lack of belonging. This doesn’t necessarily mean that hormones for trans people are always inappropriate, but the lack of credulity with which we approach folks who state that their issue is hormonal, in comparison with our general skepticism overall as a field, is baffling to me. We don’t accept a patient’s assertion that their chest pain is a heart attack without further diagnostic testing, why do we accept the assertion that their gender dysphoria is from being born in the wrong body. The relatively short follow up time in most of these studies troubles me. If you make a major change in your life that you hope will help something, your mood will go up and your suicidality will go down. I’m more interested in outcomes 3, 5 and 10 plus years down the road.”
“Chen 2023 [the paper cited by the original poster] should be a causing a sea change even on the skeptical side of the aisle. We should no longer be asking ‘Are the long term fertility risks and other risks worth the short term benefits of GAH?’ But rather we should be asking ‘Does GAH even work in the short term?’
“From an Ob-Gyn perspective, it has always concerned me the lack of focus on whether or not minors can consent to medications that may severely limit or eliminate their reproductive options later in life. In any patient who I counsel regarding permanent forms of contraception, it is always a very careful process. Additionally, even just for a salpingectomy (where actually patients technically still have the ability to get IVF, so their fertility options are not completely eliminated) Medicaid requires special consent forms signed 30 days before we can even do the surgery, after which time we only have a 6 month window. This is a protective measure to prevent patient coercion. So as giving puberty blockers and then cross sex hormones which prevent sexual maturity is a decision that I am not sure a preadolescent has the ability to consent to, from a reproductive standpoint.”
“Psychiatrist pitching in, copying over a comment from r/Psychiatry. I do not see patients who are outright MtF [Male to Female] or FtM [Female to Male] in my outpatient practice very often, and when I do it is not for their gender issues specifically, but I do see many young people these days who are gender non-conforming in some way. I have several patients who go by ‘she/they’ pronouns who are entirely unable to articulate why they prefer this to “she/her” apart from some extremely vague discomfort with entirely feminine pronouns. I am of course happy to accommodate whatever pronouns they like but it does make me wonder how much of this is social contagion combined with a generalised ‘feeling uncomfortable in your own body’ which is entirely normal for those of a certain age group or with certain other (non-gender dysphoria) mental health concerns which would simply self-terminate if not labelled and reinforced.
“Medicine being cavalier about some new intervention for a few years then starting to beat a retreat as the harms surface is a tale as old as time. These treatments are already being curtailed in Europe, we’re firmly in the retreat stage. See you in 10 years for the next big boom and bust cycle.”
The comment with the greatest number of upvotes notes that it has become so politically taboo to even ask questions “that a meaningful discussion cannot be had.”
Doctors certainly have concerns and questions. Let’s hope the Endocrine Society and American Academy of Pediatrics change their mind about hearing them.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_138847340-scaled.jpg17002560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-08-07 16:23:532026-05-11 13:05:19Reddit Discussion Reveals How Doctors Really Feel About Pediatric Gender Medicine
The Supreme Court just said racial discrimination isn’t allowed in college admissions. So how is the Association of American Medical Colleges responding to the end of affirmative action? You guessed it: By calling for more racial discrimination.
The AAMC made this factclear last week in a post focused on how to help “medical schools boost racial diversity in the wake of the Supreme Court ruling.” It wants medical schools to continue looking at their student bodies through the lens of skin color. The transparent goal is to discriminate against some races in favor of others, sacrificing merit in the process.
The AAMC writes:
Nothing in the Supreme Court decision compels us to deviate from our goal of diversifying the health care workforce,” David Skorton, CEO of the AAMC, said during a webinar with medical school leaders this month.
Figure 1. From a webinar hosted by the Association of American Medical Colleges on July 10, 2023.
In other words, racial discrimination shouldn’t go anywhere. The AAMC lists specific strategies that, it hopes, will let medical schools get around the Supreme Court’s ruling. The list includes:
“Holistic review,” in which a medical school considers the “whole applicant,” a subjective process that makes it easier to conceal the consideration of race.
“Considering essays to evaluate character strengths, career aspirations, or commitments to the school’s mission areas in ways that might include experiences or perspectives related to the applicant’s race.”
“Expanding recruitment to, or building relationships with, undergraduate institutions and community-based organizations with high levels of diversity” (translation: high levels of certain racial groups).
“Considering background factors tied to the school’s mission,” including coming from an underserved community or speaking multiple languages at home.
“Allowing student groups to encourage people from specific populations to apply to medical school.”
Separately, the AAMC has said it will continue to send applicants’ racial data to medical schools via its application service. It remains to be seen whether the AAMC will let applicants decline to disclose their race, as other services, like the Common App, are doing.
In every instance, the AAMC is doing an end-run around the Supreme Court. The Court made clear that race can’t be a factor in admissions, including at medical school. The AAMC is so radicalized, it refuses to accept that.
This cannot stand. At Do No Harm, we’re going to keep calling attention to medical schools’ racial discrimination – and absurd workarounds will not stand up in court. It’s time to get race out of medical school admissions for good.
Is your medical school still looking at race in admissions? Please let us know – securely and anonymously.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1023107128-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-08-03 18:21:112026-05-11 13:06:54AAMC: Medical Schools Should Keep Discriminating
Today, Do No Harm and Dr. Marilyn Singleton joined Dr. Azadeh Khatibi in a lawsuit challenging California’s mandatory implicit bias training for physicians to restore free speech in medical training.
Azadeh Khatibi, et al. v. Kristina Lawson, et. al, filed by the Pacific Legal Foundation, challenges mandate AB 241 passed by California lawmakers in 2019, which requires all continuing medical education (CME) courses involving direct patient care to include implicit bias training.
“Physicians have free will and act in the best interest of their patients,” said Dr. Stanley Goldfarb, Do No Harm Chairman. “The idea of unconscious bias states that one acts on those biases, and there’s no evidence of this happening in the medical community. Medical professionals take the Hippocratic oath to do no harm, and do not need lawmakers or medical organizations to tell them what they should think when providing medical advice to patients.”
According to the lawsuit, continuing medical education instructors in California are required to adopt an ideology that is unpersuasive nor unsupported by evidence to presume all healthcare providers are infected with implicit bias and thus treat patients differently.
“The implicit bias requirement promotes the inaccurate belief that white individuals are naturally racist,” said Dr. Marilyn Singleton, a visiting fellow of the Do No Harm organization and California anesthesiologist who teaches continuing medical education courses in California. “This message can be detrimental to medical professionals and their patients as it creates an atmosphere of suspicion and animosity, which goes against the fundamental principle of doing no harm.”
All California physicians must log 50 CME hours every two years as a condition of license renewal. This is a growing trend across the country as more states require implicit bias training as a condition for obtaining and retaining medical and nursing licenses.
“Physicians should base medical care on each patient’s individual situation and condition,” said Caleb Trotter, an attorney at Pacific Legal Foundation. “Implicit bias training does the opposite, telling doctors they should be concerned about a patient’s immutable characteristics like race, gender, and sexual orientation, regardless of the characteristics’ relevance to the patient’s treatment.”
The case Azadeh Khatibi, et al. v. Kristina Lawson, et. al, was filed in the U.S. District Court for the Northern District of California.
About Do No Harm
Do No Harm is a diverse group of physicians, healthcare professionals, medical students, patients, and policymakers united by a moral mission: Protect healthcare from a radical, divisive, and discriminatory ideology. They believe in making healthcare better for all – not undermining it in pursuit of a political agenda. Learn more at www.donoharmmedicine.org
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200rededge-rachelhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngrededge-rachel2023-08-01 17:31:322026-02-11 15:33:35Do No Harm joins lawsuit to challenge California’s mandatory implicit bias training in healthcare
The Journal of the American Medical Association (JAMA) recently made waves by publishing junk sciencein one of their journals. Old habits die hard. Only one week later, they’re at it again.
The new study inquires whether “implicit bias” is associated with “disparities in breast reconstruction rates, complications, or cost” among women who received mastectomies as a treatment for breast cancer.
Implicit bias refers to supposedly unconscious prejudice that affects attitudes and behaviors toward others. The “science” behind it is tenuous. The test most frequently used to measure implicit bias (including in this new study) is called the Implicit Association Test (IAT). The IAT demonstrates poor levels of reliability, meaning that outcomes tend to be volatile when the same person takes the test multiple times. The IAT also doesn’t appear to predict “biased behavior,” which ought to invite healthy skepticism about whether it measures what it purports to measure.
For woke scholars, however, it is a given that implicit bias is not only real but measurable and profoundly determinative. In this case, the “researchers” task readers to imagine that it plays a role in how doctors treat women with breast cancer and the costs associated with that care.
Precisely why “implicit bias” would lead to differences in cost or the incidence of breast reconstruction is never explained. Surgical reconstruction is a decision made by patients, so their theory compels the belief that patient agency is somehow shaped by the forces of racism.
The researchers assert that average IAT scores across regions are a functional measure of implicit bias for surgeons in that region. To test their hypothesis, they observe the degree to which implicit bias correlates with racial differences in breast reconstruction rates, complications, and costs across these Census regions.
The theory behind the study is flimsy, but the technical execution is worse. Among the myriad problems with technical execution: Featuring US Census regions as the unit of analysis means that their sample size is 9 units. It’s simply too little data to draw any meaningful inference from quantitative analysis.
Using regions as the unit of analysis also means that surgeon “implicit bias” is measured with enormous imprecision. Even if one accepts that the IAT represents a quality measure of implicit bias, the assumption that implicit bias among surgeons varies in the same way that it does among the general population in these regions represents a methodological leap of faith.
Moreover, it turns out that there is almost no variation in IAT score by Census region. Whereas results in IAT score can range from -2 to 2, scores among the 9 regions range from 0.29 to 0.33.
The fact that their study consists of 9 observations and an outcome with almost no variation means that it was all but predetermined that the researchers would not observe statistically significant results, and indeed they do not. Nevertheless, the researchers conclude that “efforts to reduce the observed inequities” – which they did not observe – “should remain a national priority… efforts from individual institutions and national surgical organizations are needed to provide culturally competent, evidence-based care to individuals of all racial and ethnic backgrounds.”
A great deal of postmodern woke “scholarship” features researchers manipulating data to arrive at a preferred outcome or overstating findings. The authors of this new study appear to lack the technical skill needed to do that. Instead, when the analysis does not support their conclusion, they simply provide the same canned policy recommendations that they would have provided if their analysis did support their hypothesis. In other words, JAMA has become so tendentious that its debased standards now apparently allow researchers to perform dog and pony analysis instead of empirical sleight of hand.
Ultimately there is only one lesson to be drawn from the new study: Go woke, go intellectually broke.
Ian Kingsbury is the Director of Research for Do No Harm.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1023401932-1-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-08-01 12:49:222026-05-11 13:08:07JAMA Beclowns Itself Yet Again
Grand rounds traditionally provide medical professionals with helpful information presented by clinical experts. But the Icahn School of Medicine at Mt. Sinai (ISMMS) used a recent grand rounds session as a platform to perpetuate divisiveness and incorrect assumptions.
Figure 1. Flyer promoting the Medical Education Grand Rounds presentation at Icahn School of Medicine on April 18, 2023.
The Institute for Medical Education at ISMMS hosted Dr. Dowin Boatright for an April 18, 2023 presentation of Exploring the Experiences of Historically Excluded Students in the Medical School Learning Environment and the Impact of Those Experiences.
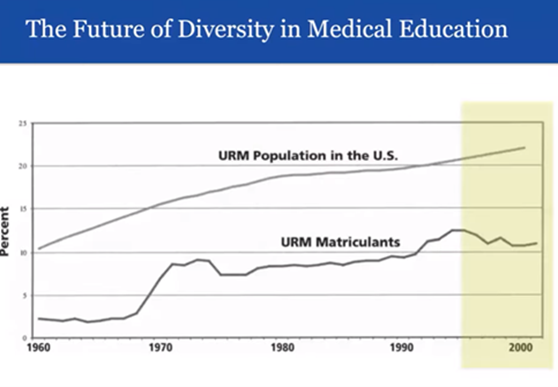
After presenting statistics regarding the care of non-white and non-English-speaking patients and “diversity’s influence on medical education,” Dr. Boatright began speaking about “declines in the diversity of medical school matriculants.” To make this point, he cited information on “URM matriculants” from the mid-1990s. He attributed these declines to “additional cases nationally challenging affirmative action.”
Figure 2. From ISMMS Medical Education Grand Rounds presentation by Dr. D. Boatright (April 18, 2023).
Dr. Boatright warned that “another period of stagnation” for diversity in medical school admissions with “very high-profile Supreme Court cases challenging affirmative action” was on the horizon. He is referring to the Harvard and University of North Carolina cases, brought by Students for Fair Admissions (SFFA). These cases challenged the Constitutionality of race-based admissions in higher education and argued that discriminating against applicants based on skin color violates the Civil Rights Act of 1964.
For decades, the Supreme Court allowed public and private universities – including medical schools – to perpetuate such discrimination under the guise of “affirmative action.” This essentially told the schools that racial discrimination, done in the name of increasing diversity, was legal. On June 29, 2023, the Court affirmed that our Constitution and laws are color-blind and that every person is equal under the law. The rulings mean that universities must not discriminate against applicants based on race/ethnicity, including medical schools, when considering applicants for admission.
Dr. Boatright further defended his position by stating that the downward trend continued until the Liaison Committee on Medical Education (LCME), which oversees accreditation of medical schools, “began to exert its own influence on diversity.” He referred to two 2009 standards from the LCME (MS-8A and IS-16), pointing out that they use the word “must” regarding the development of programs and policies aimed at increasing diversity in medical school admissions.
“For the first time, medical schools were required to have programs and practices in place to have diverse students, faculty, and residents, and to retain those individuals. And if they didn’t,” Dr. Boatright continued, “and meet subsequent criteria, those medical schools could be cited by the LCME and ultimately lose their accreditation.” He did not indicate which, if any, medical schools have received such a citation or were at risk of losing their accreditation for failing to implement diversity initiatives.
There is a good reason for that. As noted in a Wall Street Journal editorial on July 25, 2023, the LCME itself confirmed that its diversity requirements are not the rigid mandates that professors like Dr. Boatright assumed. “In a letter responding to a questionnaire from the House Committee on Education and the Workforce,” the WSJ piece reported, “LCME says that ‘nothing’ in the text ‘mandates which categories of diversity a medical school must use to satisfy this element.’”
https://youtu.be/Bn4ab2QHTXQ
VIDEO: From Exploring the Experiences of Historically Excluded Students in the Medical School Learning Environment and the Impact of Those Experiences by Dr. Dowin Boatright (April 18,, 2023).
Dr. Boatright is known as being one of three physicians who published Blackface in White Space: Using Admissions to Address Racism in Medical Education (October 2020). The authors’ claim? “[T]hat most medical schools are white spaces where explicit and implicit racism occurs constantly and often goes unmentioned and unpunished.”
Figure 3. From “Blackface in White Space: Using Admissions to Address Racism in Medical Education” (July 29, 2020).
Boatright and his co-authors voiced a clear directive: “Stop admitting applicants with racist beliefs.” Among the recommendations for admissions officers to take was secondary essay prompts, which “could be enhanced to more clearly elicit applicants’ positions on race.” As we reported last year, secondary interview questions that address the topics that Boatright supports are a means to identify accepters and dissenters of the health equity and social justice initiatives of several medical schools.
The Icahn School of Medicine at Mt. Sinai is forthcoming about its goals for achieving “anti-racist transformation in medical education,” and hosting Dr. Boatright and his message aligns with those goals.
However, propagating racial divisiveness and unsubstantiated claims about medical school admissions and accreditation in the name of grand rounds is intellectually dishonest and contributes nothing to the professional development of busy physicians. If anything, the Harvard and UNC cases he bemoans exposed racially discriminatory policies in the admissions process and have ended the practices that ISMMS and Dr. Boatright endorsed. We applaud the Supreme Court’s rulings and will continue to pursue the restoration of merit to the admissions process in all medical schools, including ISMMS.
Are you seeing ideology invading the grand rounds sessions at your institution? Do No Harm wants to hear from you, and you may remain anonymous if you wish.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_152077328-scaled.jpg16972560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-07-29 12:45:332026-05-07 16:27:27Speaker at the Icahn School of Medicine at Mt. Sinai Blames Civil Rights Legal Cases For “Declines In Diversity of Medical School Matriculants”
American medical associations profess certainty about the wisdom of medical transition for kids, but European countries are urging caution and publicly rebuking American standards of care. It begs the question: What do American doctors know that European doctors don’t?
In a letter published in the Wall Street Journal (WSJ), parents of gender questioning youth join the chorus of those demanding an answer.
The question from twelve parents of once or current gender-questioning youth comes in response to a conversation initiated by Do No Harm. After attending the Endocrine Society’s annual meeting, we published a WSJ op-ed revealing that the consensus projected by the Endocrine Society on pediatric medicine is illusionary. Many doctors express deep misgivings about current practices and the absence of evidence to support them. In response, Endocrine Society President Stephen Hammes published a WSJ letter doubling down on the position that current guidelines are backed by evidence and consensus. That earned him a rebuke from an international group of experts, who accused Hammes of “politicizing” the issue and “exaggerating the benefits and minimizing the risks” of medical transition.
The letter from parents expresses “concern” about “the Endocrine Society’s unwillingness to acknowledge this growing consensus against its preferred approach.” It also expresses concern that Dr. Hammes did not reveal his position as “a co-director of a transgender clinic that administers hormonal interventions to teenagers—a potential conflict of interest.”
Parents of kids who have expressed confusion about gender are often told by healthcare providers – without justification – that failure to medically affirm could culminate in the child’s suicide. In some disturbing cases parents have even lost custody of their kids for disagreeing about medical transition. That includes Ted Hudacko, one of the signatories of the new letter.
If Mr. Hudacko lived in the U.K., Sweden, or Finland, his son would have received psychotherapy. Instead, his son received irreversible medical treatments and a broken family. Ted and other parents deserve to know why.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_535653202-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-07-27 22:36:422026-05-07 16:29:52Parents of Gender Diverse Children Demand Answers from Endocrine Society
On July 27, 2023, Do No Harm senior fellow and patient advocate Chloe Cole testified before The House Judiciary Subcommittee on the Constitution and Limited Government at the hearing titled “The Dangers and Due Process Violations of ‘Gender-Affirming Care’”.
Here are Chloe’s remarks:
Hi, I’m Chloe Cole and I am a detransitioner. Another way to put that would be: I used to believe I was born in the wrong body, and adults in my life whom I trusted affirmed my belief, causing me lifelong, irreversible harm. I speak to you today as a victim of one of the biggest medical scandals in the history of The United States of America. I speak to you in the hope that you will have the courage to bring this scandal to an end and ensure that other vulnerable teenagers, children, and young adults don’t go through what I went through.
At the age of 12 I began to experience what my medical team would later diagnose as gender dysphoria. I was well into puberty and I was very uncomfortable with the changes that were happening to my body. I was intimidated by male attention and when I told my parents I felt like a boy, in retrospect all I meant was that I hated puberty, that I wanted this newfound sexual attention to go away, that I looked up to my brothers a bit more than to my sisters.
I came out as transgender in a letter I set on the dining room table. My parents were immediately concerned. They felt like they needed to get outside help from medical professionals. This proved to be a mistake. It immediately set our entire family down a path of ideologically-motivated deceit and coercion.
The gender specialist I was taken to see told my parents that I needed to be put on puberty blocking drugs right away. They asked my parents a simple question: “Would you rather have a dead daughter, or a living transgender son?”
https://youtu.be/F-pge2z6bsU
Chloe Cole testifying before the House Judiciary Subcommittee on Crime and Federal Government Surveillance on July 27, 2023.
The choice was enough for my parents to let their guard down, and in retrospect I can’t blame them. This was the moment we all became victims of so-called “gender-affirming care.” I was fast tracked onto puberty blockers, and then testosterone. The resulting menopausal-like hot flashes made focusing on school impossible. I still get joint pains and weird pops in my back but they were far worse when I was on the blockers.
A month later, I was 13 and had my first testosterone injection. This caused permanent changes to my body. My voice will forever be deeper, my jawline sharper, my nose longer, my bone structure permanently masculinized, my Adams apple more prominent, and my fertility unknown. I look in the mirror sometimes and feel like a monster.
I had a double mastectomy at 15. They tested my amputated breasts for cancer, I was cancer free, of course; I was perfectly healthy. There was nothing wrong with my still developing body or my breasts other than that, as an insecure teenage girl, I felt awkward about it. After my breasts were taken away from me they were incinerated. Before I was able to legally drive I had a huge part of my future womanhood taken from me. I will never be able to breastfeed. I struggle to look at myself in the mirror at times. I still struggle to this day with sexual dysfunction, and I have massive scars across my chest. The skin grafts that they used – that they took of my nipples – are weeping fluid today. They were grafted into a more “masculine position,” they said.
After surgery my grades in school plummeted. Everything that I went through did nothing to address the underlying mental health issues that I had. My doctors, with their theories on gender, thought that all my problems would go away as soon as I was surgically transformed into something that vaguely resembled a boy. Their theories were wrong. The drugs and surgeries changed my body but they did not, and could not, change the basic reality that I am, and forever will be, a female.
When my specialist first told my parents that they could have a dead daughter or live transgender son, I wasn’t suicidal. I was a happy child who struggled because she was different. However, at 16, after my surgery, I did become suicidal. I am doing better now, but my parents almost got the dead daughter promised to them by my doctors. My doctors had almost created the very nightmare they said they were trying to avoid.
So, what message do I want to bring to American teenagers and their families? I didn’t need to be lied to, I needed compassion. I needed to be loved. I needed to be given therapy to help me work through my issues, not affirmed in my delusion that transforming into a boy would solve my problems.
We need to stop telling 12-year-olds that they were born wrong, that they are right to reject their own bodies and feel uncomfortable in their own skin. We need to stop telling children that puberty is an option, that they can choose what kind of puberty they will go through just as they can choose what clothes to wear or what music to listen to. Puberty is a rite of passage to adulthood, not a disease to be mitigated.
Today, I should be at home with my family celebrating my 19th birthday. Instead, I am making a desperate plea to my elected representatives. Learn the lessons from other medical scandals like the opioid crisis, to recognize that doctors are human too, and sometimes they are wrong.
My childhood was ruined along with thousands of detransitioners that I know through our networks. This needs to stop. You alone can stop it. Enough children have already been victimized by this barbaric pseudoscience. Please let me be your final warning. Thank you.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2310926035-scaled.jpg18262560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-07-27 18:37:402026-05-07 16:31:16Do No Harm Senior Fellow Chloe Cole Testifies Before Congress
That’s the message state lawmakers received on July 25th. Since the start of this year, they’ve been told that getting divisive and discriminatory woke ideology out of medical schools would jeopardize the schools’ accreditation. The threat stopped necessary reforms in multiple states, including Missouri, Utah, and Tennessee. But the threat isn’t real, as the main accreditor has now made clear.
This clarity comes courtesy of the House Committee on Education and the Workforce, led by Rep. Virginia Foxx. The committee asked the Liaison Committee on Medical Education, which accredits medical schools, to explain what its “diversity standards” really mean. The Wall Street Journalbroke the LCME’s response to the committee:
LCME is now [signaling] its diversity requirement is not as inflexible as schools have assumed. In a letter responding to a questionnaire from the House Committee on Education and the Workforce, LCME says that “nothing” in the text “mandates which categories of diversity a medical school must use to satisfy this element.”…
That’s an opening for Missouri, Tennessee, Utah and other states looking for ways to get the DEI bureaucracy out of medical schools. The Missouri Legislature considered a bill that would have banned schools from “conducting DEI audits” or hiring DEI consultants, but it later backed off for fear the schools wouldn’t be able to comply with both state law and the rules of the national accreditor.
The LCME also disavowed pursuing any so-called “anti-racism efforts,” which despite the name, require racial discrimination. The LCME also denies that America is systemically racist, and it doesn’t require medical schools to teach such a lie.
The message to state lawmakers couldn’t be more clear: There’s nothing blocking them from getting woke ideology out of medical schools. Now that this threat is off the table, every state should pass sweeping reforms as soon as possible. Medical students – and the patients they will eventually treat – deserve swift action.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2219213657-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-07-27 01:15:122026-05-07 16:32:43States Can Ditch DEI At Medical Schools
Kansas City, watch out. The American Academy of Family Physicians is preparing to hold its 49th National Conference of Medical Students there. Before that happens, one of its executives has a message: Discrimination and division are good for medicine.
That’s the takeaway from a letter in the Kansas City Star by Karen Mitchell, the Academy’s Vice President of Medical Education. She laments the Supreme Court’s recent rejection of affirmative action, while calling on medical schools and policymakers to find new ways to discriminate by race and indoctrinate students and physicians.
Ms. Mitchell should ask patients what kind of physician they want to see. The answer will always be the best physician possible, not someone who was hired because of their skin color or someone who was trained to be a political activist. When the Supreme Court ended affirmative action, which medical schools have used for decades, it opened the door to recruiting students based on merit. Equal treatment under the law is essential to the quality of the future physician workforce.
The Academy should be supporting, not opposing, merit in medical education. It should also be supporting legislation that gets divisive and discriminatory ideology out of medical schools. Bills to that effect nearly passed in both Kansas and Missouri this spring. They deserve to be brought back up and signed into law as soon as possible.
For that matter, as Kansas City prepares to host the National Conference of Medical Students, residents should ask the American Academy of Family Physicians to explain why it’s so focused on race. You’d think it would be more concerned with ensuring that every patient gets the best physician and best possible care. That’s what patients in Kansas City and everywhere else deserve, even if it’s not what medical elites want.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2225540011-scaled-e1778186080855.jpg8531254Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-07-27 00:48:012026-05-07 16:34:53When Family Physicians Forget Their Principles
The University of Southern California (USC) Keck School of Medicine has made significant changes in the eligibility criteria for a discriminatory program as the result of a federal civil rights complaint and subsequent investigation.
In late 2022, we reported that the U.S. Department of Education’s Office for Civil Rights (OCR) had opened a federal civil rights investigation of the USC Keck School of Medicine for its Diversity in Medicine Visiting Clerkship. Mark Perry, senior fellow at Do No Harm, filed a complaint last August against this program for illegal race-based discrimination in violation of Title VI of the Civil Rights Act of 1964.
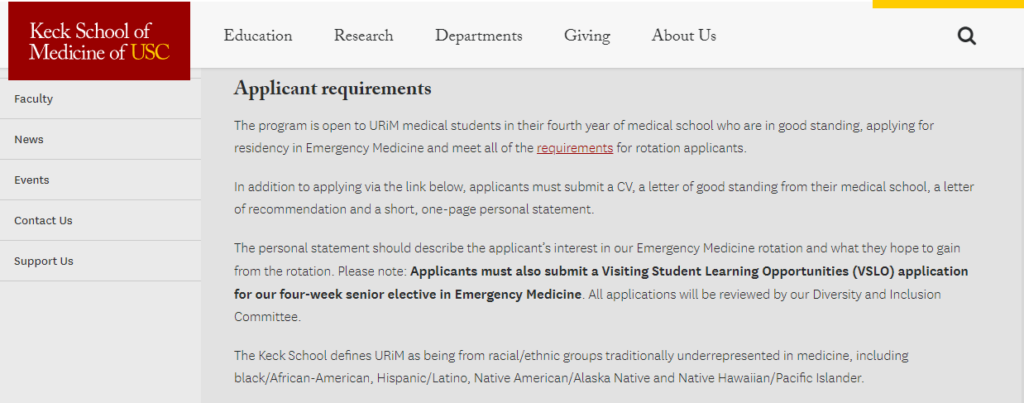
The previous version of the program said it supports fourth-year medical student groups who are “traditionally underrepresented in medicine (URiM).” The USC Keck School of Medicine defined URiM as “black/African-American, Hispanic/Latino, Native American/Alaska Native, and Native Hawaiian/Pacific Islander.”
Figure 1. USC Keck School of Medicine Diversity in Medicine Visiting Clerkship Award webpage as it appeared on January 31, 2023.
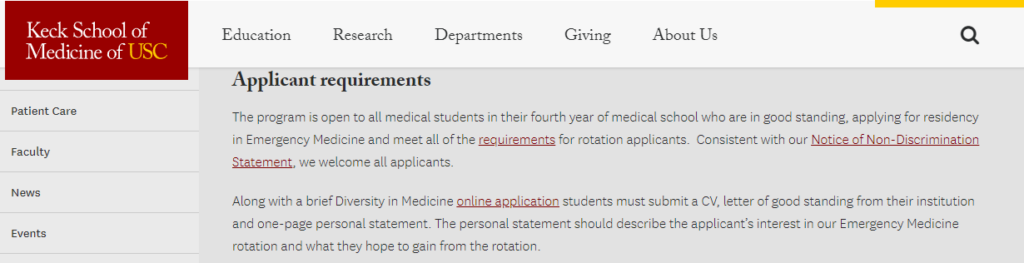
The current version of the program shows that the race-based eligibility has been removed, and the clerkship is now open to all fourth-year medical students in good standing. “Consistent with our Notice of Non-Discrimination Statement,” the site states, “we welcome all applicants.”
Figure 2. USC Keck School of Medicine Diversity in Medicine Visiting Clerkship Award webpage as it currently appears.
The associated application does not ask for race/ethnicity, but does request a student’s “chosen pronoun.” The previous version of the clerkship did not refer to this application.
The OCR has informed Perry last week that the investigation into USC’s Keck School of Medicine has been resolved due to the revisions made following the opening of the investigation last December. “Since then, the University has revised the language on the webpages to indicate that the Award is targeted at medical students from diverse backgrounds,” the OCR said, “including students who are underrepresented in medicine, but is not restricted by race or ethnicity.”
“Overall, I would say that it’s a pretty thorough correction of USC’s Title VI violation,” Perry said, “and is exactly the type of correction we are looking for when we challenge a medical school’s legally indefensible racial discrimination.”
Have you seen fellowships or scholarships in U.S. universities with healthcare education programs that discriminate on the basis of race/ethnicity or sex? Do No Harm wants to hear from you.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1957533307-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-07-26 21:12:212026-05-07 16:36:37USC Keck School of Medicine Makes Substantial Corrections in Response to Federal Civil Rights Investigation
Cincinnati Children’s Hospital Medical Center (CCHMC) is dedicated to injecting the diversity, equity, and inclusion (DEI) dogma into every area of its patient care, education, and research operations.
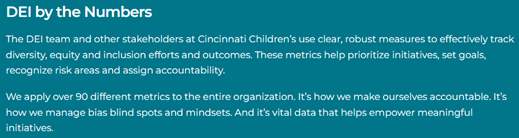
A visit to the website of Cincinnati Children’s displays the facility’s commitment to DEI as “fundamental to who we are” and features its “first DEI Annual Report.” A graphic on this page shows that CCHMC applies more than 90 DEI metrics across the entire organization, which are highlighted throughout the 28-page report.
Figure 1. Cincinnati Children’s Diversity, Equity, and Inclusion webpage.
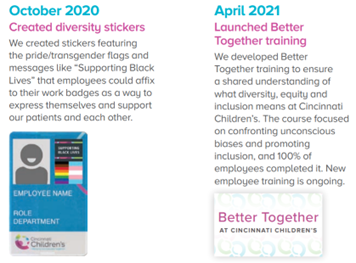
CCHMC promises “a unified, unwavering focus on DEI” to strengthen its mission, as the report clearly demonstrates by illustrating the “DEI journey.” Once the organization “declared racism a public health crisis” in July 2020, a five-year DEI Strategic Plan (approved by the Board of Trustees) was created to “embed DEI in every aspect of our work.” Employees were provided with “diversity stickers” and focused training to ensure they understood what DEI means and how to confront their unconscious biases.
Figure 2. CCHMC DEI Annual Report, p. 4.
The “diversity infrastructure” was further reinforced by forming a Diversity Council, steering committees, and Employee Resource Groups (ERGs), adopting the use of preferred pronouns, establishing a center for “child health equity,” and posting a “formalized DEI scorecard.”
Figure 3. CCHMC DEI Annual Report, p.13.
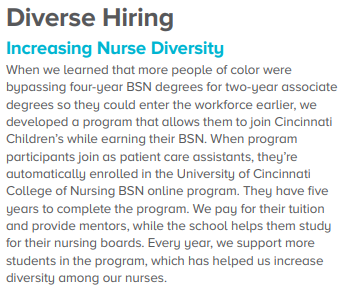
The DEI scorecard is updated on a quarterly basis to discover where goals are and are not being met, such in CCHMC’s hiring practices. “When we learned that more people of color were bypassing four-year BSN degrees for two-year associate degrees so they could enter the workforce earlier,” the report said, we developed a program that allows them to join Cincinnati Children’s while earning their BSN.” The program pays for tuition at the University of Cincinnati College of Nursing and provides mentors – however, eligibility is based on skin color.
Figure 4. CCHMC DEI Annual Report, p. 15.
But the organization doesn’t limit its indoctrination efforts to the patient care space. This year, CCHMC has sustained the DEI doctrine through ongoing education efforts. Its InterProfessional Continuing Education (IPCE) program published the DEI Guide for Health Educatorsto direct them on how to “create content and learning environments that promote diversity, equity, and inclusion.” The online guide, distributed in the January 2023 edition of the IPCE Central Newsletter, provides “general DEI principles” to apply in the development of continuing education offerings, including considerations and cautions for the educator to heed, such as:
Avoid overuse of traditional images of medical professionals and patients. For example: physicians as white men, nurses as white women, patients as people of color.
In hypothetical case scenarios, only highlight aspects of a person’s identity if it is relevant and meaningful. For example, mentioning a patient’s race in relation to systemic racism and inequitable access to mental health resources is appropriate. Mentioning a patient’s race in an attempt at showing diversity is “tokenism” and depending on the scenario can reinforce stereotypes.
Focus on the person first, not their disability/diagnosis. Describe what the person has, not who the person is. Instead of “child is learning disabled,” say “child has a learning disability.”
Use all demographics included in a research study and consider if any intersecting identities correlate to the results.
The guide offers additional direction in eleven “deep dive” categories that “are often associated with marginalization in healthcare and healthcare education.” The considerations and cautions in these sections address elements such as “intersectionality” and “bias awareness and microaggressions.”
Figure 5. Deep Dive Categories in the DEI Guide for Health Educators.
For example, in the “Sex, Gender, & Sexual Orientation” section, educators are advised to:
Use they/them pronouns when referring to individuals whose gender is unknown or hypothetical characters in case examples whose gender is not relevant to the discussion.
Refer to individuals by their affirmed gender and pronouns – the gender and pronouns by which they wish to be known.
Avoid unnecessarily gendering items. Instead of “feminine hygiene products,” say “menstrual products.”
Recognize the importance of acknowledging both medically necessary sex information while still respecting gender identity. For example: a menstruating person.
Figure 6. From the Cincinnati Children’s DEI Guide for Health Educators.
Cincinnati Children’s Hospital invests in the advancement of DEI concepts and gender ideology, and is proud to display its woke credentials to patients, staff, and the public. But the health of Ohio’s children is better served by devoting scarce resources to developing and training staff members in models of care that are based on science and the best available evidence.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1036592035-scaled.jpg17082560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-07-20 21:43:162026-05-07 16:38:12DEI Indoctrination For All at Cincinnati Children’s Hospital
Virginia children are safer now than they were last week. That’s the reality of new policies from Virginia Gov. Glenn Youngkin protecting children from transgender activism, especially in the context of public education. Other states should pay attention to these policies – and ideally, pass similar laws or regulations of their own.
Gov. Youngkin is undoing the damage of his predecessor, Gov. Ralph Northam. The Northam administration essentially gutted parents’ rights to have a say in their child’s medical care, especially in cases where school officials try to help children change gender. The Northam approach made it easier for children to obtain sex-change counseling and ultimately treatments, which lead to a lifetime of mental and physical health challenges.
Not anymore. Gov. Youngkin’s policies require schools to tell parents if their children are experiencing gender-related issues. Schools are prohibited from concealing information from parents, and before a child can use different pronouns, parents must consent. While the policies aren’t perfect, they represent a giant leap in the right direction.
Practically, these policies will stop radical activists from pushing children – whose minds aren’t fully developed – down a dangerous road of sex-change drugs and surgeries. And the empowerment of parents is especially praiseworthy. Parents should be involved in decisions about their children, especially when it comes to medical care. No one should deny them their rights or keep them in the dark.
Virginia’s move comes as a growing number of states enact policies to protect children from invasive and irreversible sex-change treatments. More and more European countries are also rolling back transgender treatments, recognizing that they do more harm than good. Kudos to Gov. Glenn Youngkin for putting common sense and science ahead of transgender ideology.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1206730276-scaled.jpg17092560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-07-20 20:44:582026-05-07 16:46:10Gov. Youngkin Protects Virginia Children
That’s the undeniable reality of a letter published last week in the Wall Street Journal by 21 clinicians and researchers from nine countries.
The authors, including some of the foremost experts in pediatric gender medicine, warn that childhood medical transition carries uncertain evidence of benefit but “the risks are significant and include sterility, lifelong dependence on medication and the anguish of regret.”
The letter directly contradicts a recent letter from Dr. Stephen Hammes, President of the Endocrine Society. Writing in response to a letter from Do No Harm, Hammes erroneously claimed that supposed mental health benefits of childhood medical transition are supported by robust evidence. The 21 experts rebuke that assertion in concluding that medical societies should “align with their recommendations with the best available evidence—rather than exaggerating the benefits and minimizing the risks.”
The new letter marks a critical milestone in the pediatric gender medicine debate for a couple of reasons. First, it provides further evidence that pediatric gender medicine is not based on consensus organically forged through open inquiry. Rather—like the Do No Harm letter that initiated this conversation notes—it is an illusion sustained through activist capture of medical societies and the suppression of dissent.
More importantly, the letter amounts to inconvertible evidence that trans activists have been lying about Europe’s reckoning with childhood medical transition. Activists recognize how politically damning it would be to acknowledge that some of the world’s most progressive countries are urging caution on pediatric gender medicine, so they claim that recent changes in Europe are simply procedural and not animated by concerns around over-treatment.
In reality, Sweden, Finland, and the U.K. have conducted systematic reviews of the safety and efficacy of pediatric gender medicine and concluded that it isn’t clear that risks exceed benefits. The Swedish review in fact concluded that the risks of puberty blockers exceeded the benefits. All three countries have restricted the use of puberty blockers to clinical research settings and the most exceptional cases of dysphoria.
Authorities in France and Ireland have also raised recent concerns about the use of puberty blockers as a treatment for childhood gender dysphoria.
The U.S. is an outlier in the extent to which the healthcare establishment professes certainty about the wisdom of pediatric gender medicine. Thanks to the courage and candor of these 21 experts, even activists will be forced to admit as much.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2173526753-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-07-17 15:58:552026-05-07 16:47:40Taking Stock of a Milestone Moment in the Pediatric Gender Medicine Debate
The University of Florida College of Medicine (UFCOM) in Jacksonville has done some housekeeping on its website since a federal civil rights investigation into a discriminatory scholar program was opened.
In October 2022,Do No Harm senior fellow Mark Perry filed a complaint with the U.S. Department of Education’s Office for Civil Rights (OCR) regarding UFCOM Jacksonville’s Visiting Elective Scholars Program in the Department of Pediatrics (archived page here). The complaint cited violations of both Title VI and Title IX, as eligibility to apply was limited to “Individuals belonging to a group considered underrepresented in medicine (Black/African-American, Hispanic/Latino, Native American, Pacific Islander/Native Hawaiian, and LGBTQ+).”
Figure 1. Eligibility criteria for UFCCOM-Jacksonville Department of Pediatrics Visiting Elective Scholars Program (archived page).
OCR referred the case for investigation, which was opened on April 10, 2023. However, a recent review of the UFCOM-Jacksonville website shows that it has been scrubbed clean of any evidence of the program, with no indication that it has been moved to another location.
UFCOM has used this tactic before. Last November, in response to media coverage of our comprehensive report, UFCOM permanently removed divisive and ideological material from its admissions homepage and DEI-related resources.
If you are aware of a scholarship, fellowship, or other program that violates federal civil rights laws at your school or institution, please inform us. Do No Harm will conduct a review and will take appropriate action if the program is discriminating on the basis of race or sex.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_457354732-scaled.jpg17082560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-07-14 21:07:342026-05-07 16:49:29The University of Florida College of Medicine Hits the “Delete” Button on a Discriminatory Visiting Scholars Program
How will medical schools respond to the Supreme Court’s recent ban on affirmative action? Essentially every medical school practiced this race-based discrimination before the ruling. Now the man who took this issue to the Supreme Court is warning educational institutions to follow the law and do what’s right.
Edward Blum, who founded the organization at the heart of the case, has sent letters to 150 colleges and universities. As reported in the Wall Street Journal, he wrote that it is “incumbent on your institution to ensure compliance with this decision, starting with this admissions cycle.” The letters went to the schools’ presidents, deans of admission, and general counsels.
Medical schools have a choice to make. Some may try to get around the ruling by creating new race-based admissions options, such as scholarships that are restricted to people with certain skin colors. This approach violates the spirit of the ruling, and more importantly, the letter of federal law. Medical schools may also try other creative ways to continue discriminating, such as prioritizing students from gerrymandered zip codes.
This cannot be allowed. The best – and only valid – option is to treat every applicant equally, recruiting medical students based on merit. That’s what medical schools are supposed to do, not least because it leads to the best possible physicians who will provide the best possible care.
Kudos to Edward Blum for bringing this fight so far – and for continuing the fight until equality fully wins. Every American should hope this cause succeeds, and Do No Harm will do our part to ensure it happens.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_216196921-scaled.jpg17002560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-07-14 20:37:502026-05-07 16:50:50Dear Medical Schools: Don’t Defy the Supreme Court