Colorado patients, beware. The state is moving toward matching patients and physicians by race and other characteristics – a woke demand that comes down to segregation. At least two major Colorado health insurance companies are now asking providers to detail the demographic make-up of doctors and staff, setting the stage for the return of one of the worst evils in American history.
This coming fiasco has its roots in 2021, when Colorado passed a public-option law. The law led to a state regulation that requires public-option plans to “offer a culturally responsive network of providers.” The regulation also has an “action plan” if “the network does not meet these standards.” Yet “culturally responsive” is woke-speak for pushing patients to see physicians that are the same race or share other characteristics.
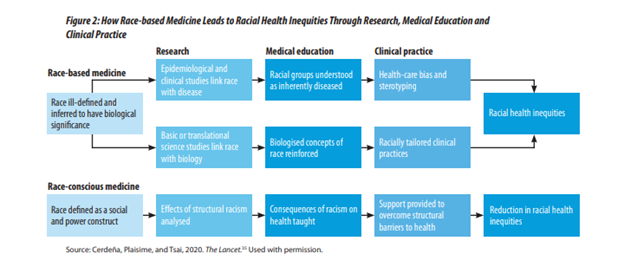
This is blatant segregation, which activists seem to know. They disguise the reality of their demands by calling it “racial concordance.” Medical journals now routinely publish articles and opinion pieces calling for racial concordance, arguing that it leads to better health outcomes. Yet the largest study on the issue, covering 56,000 patients, failed to show a benefit, and Do No Harm has conclusively proven that activists are wrong. No matter what you call it, segregation is not medically justified, to say nothing of morally justified.

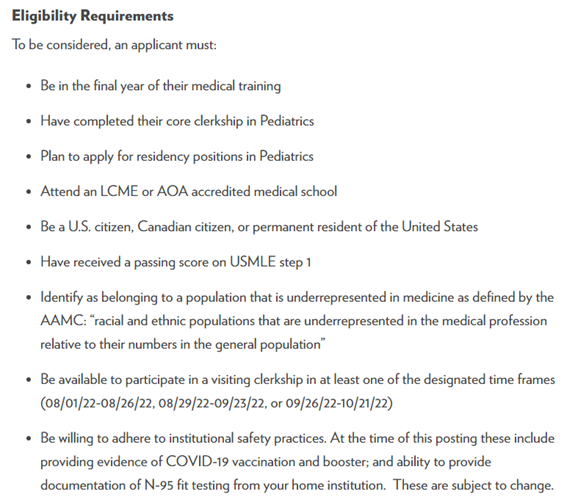
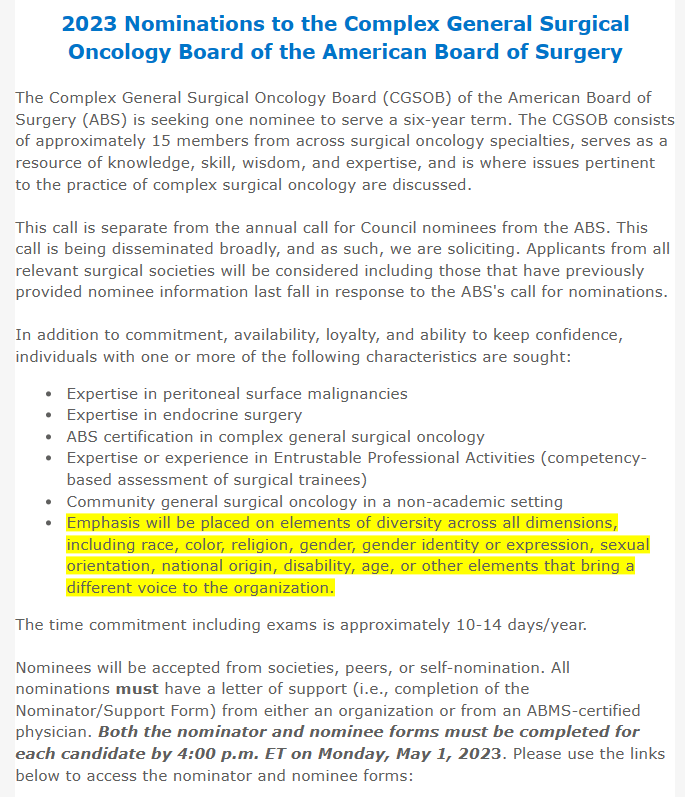
Figure 1. From Regulation 4-2-80, Section 5 (Colorado Department of Regulatory Agencies, Division of Insurance).
Anthem Blue Cross/Blue Shield is on board with this push. In a recent email to its provider network, the health insurance company has asked providers to detail their “demographic data.” It justifies this request by saying, “The demographic data will be used to improve racial health equity [and] reduce health disparities for covered persons who experience higher rates of health disparities and inequities.” Left unsaid is the means by which these supposed benefits will happen. It’s segregation.
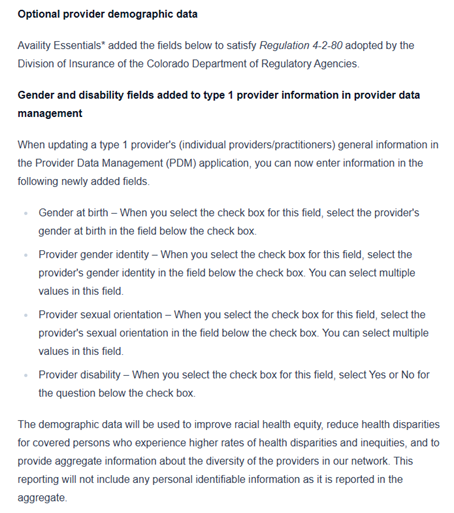
Anthem specifically wants to know about gender, gender identity, sexual orientation, and disability. Colorado also requires that Anthem and other companies ask about race and ethnicity. This seems to indicate that the segregation will extend beyond far beyond race. United Health Care, another Colorado health insurance company, has requested similar information from providers in its network.

What Colorado is doing is medically and morally wrong. Colorado shouldn’t move toward so-called “racial concordance” in health care, and health insurance companies shouldn’t go along with this travesty. Segregation has no place in health care – or anywhere else.