Forget finding the “top doctor” in your area. Castle Connolly, which publishes the famous top doctor rankings, is now interested in connecting patients with physicians based on shared race. It’s the latest example of one of the most worrisome woke trends in health care – the re-introduction of racial segregation.
A tipster sent us an email they received from Castle Connolly, asking physicians to participate in its “diversity, equity, and inclusion initiative.” The email notes that Castle Connolly has never published information about the “diversity of our network.” The initiative will fix that, with the explicit goal of connecting patients by race.
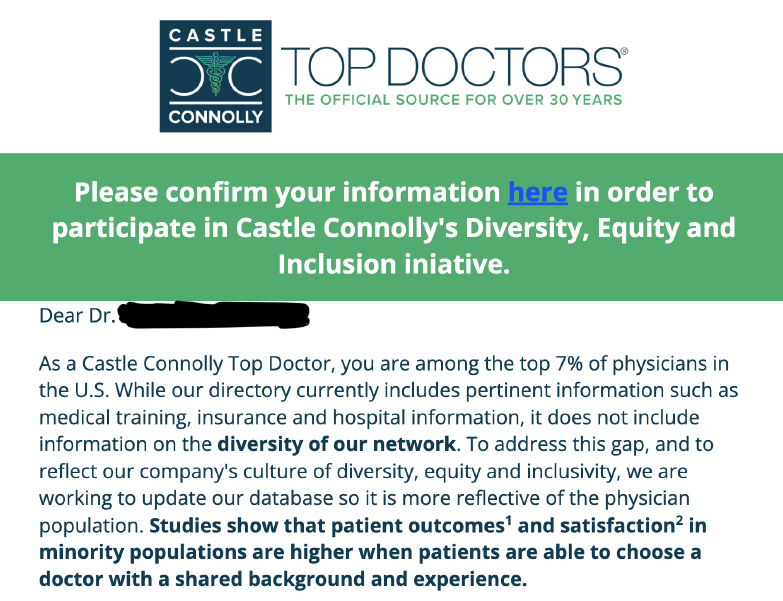
Castle Connolly justifies this move by stating that “studies show patient outcomes and satisfaction in minority populations are higher when patients are able to choose a doctor with a shared background and experience.” That’s code for the company’s desire to pair black patients with black doctors, white patients with white doctors, and so on.
Contrary to the company’s claims, there’s no good evidence supporting this policy, which is known as “race concordance.” Just the opposite: The best and largest studies show that racial concordance has no health benefits. Naturally, woke activists dispute this, and they are willing to manipulate and cherry-pick data to bolster their baseless assertion.
Castle Connolly is also ignoring that racial concordance sows seeds of distrust in the doctor-patient relationship. It discourages black patients from seeing white doctors out of fear that their health may be in danger. It does the same for white patients, who will avoid black doctors. Is this really the message the “top-doctor” company wants to send?
Patients should always be free to pick the physician that’s best for them. But companies like Castle Connolly should never push anyone into race-based doctor-patient relationships, nor should they falsely claim that such a system is better for patient health. Health care is in a bad place indeed when racial segregation is somehow seen as good for patients.