In early October, the Medical College of Wisconsin (MCW) subjected medical students to a workshop aimed at inculcating students into the DEI ideology.
The “Race Matters Workshop” was included in MCW’s “The Good Doctor” course, which is intended to instruct students on professionalism, ethics, and other soft skills in the medical workplace.
According to a description of the workshop obtained by Do No Harm, its learning objectives are replete with references to DEI and implicit bias. These objectives make clear that medical students are expected to agree with the premises of radical identity politics.
For instance, one objective is that students “[d]emonstrate knowledge of inherent biases and how they affect the way we interact with patients and advocate for them.”
There is no evidence that “implicit biases” explain racial health disparities, and the tests used to evaluate implicit bias fail to meet widely-accepted standards of reliability and validity.
For instance, a 2013 meta-analysis published in the Journal of Personality and Social Psychology found that Implicit Association Tests (IATs) were “poor predictors” of real-world bias and discrimination.
Nevertheless, other course objectives include: “Describe the role that providers have in addressing racism as a health issue in clinic settings and discuss some of the challenges and barriers faced when doing so”; and “Discuss ways that participants can be the voice for patients who are affected by health disparities created by racism.”
To be clear, it is not the role of a medical provider to serve as an activist; a physician’s goal is to provide the best possible care to his or her patients.
Moreover, redefining the responsibilities and mission of healthcare professionals so that they moonlight as “racism ombudsmen” is harmful and naturally politicizes the workplace. It erodes trust, creating a presumption that healthcare is inherently racist, and encourages healthcare professionals to adopt the premises of political ideology. It encourages providers to be on the hunt for structural boogeymen rather than focusing on promoting the good health of individual patients.
Additionally, the workshop asks students to read a resolution from the Wisconsin Public Health Association (WPHA) declaring that “Racism is a Public Health Crisis.”
The resolution states that “public health’s responsibilities to address racism include reshaping our discourse and agenda so that we all actively engage in racial justice work.”
Additionally, the resolution commits the WPHA to “creat[ing] an equity and justice oriented organization” and “identifying specific activities to increase diversity and to incorporate antiracism principles across WPHA membership, leadership, staffing and contracting.”
Other commitments include: “Advocat[ing] for relevant policies that improve health in communities of color, and supports local, state, and federal initiatives that advance social justice.”
This resolution is presumably the MCW’s model for its students: promoting DEI in the workplace, including through discriminatory means, and engaging in political activism.
But that’s not all.
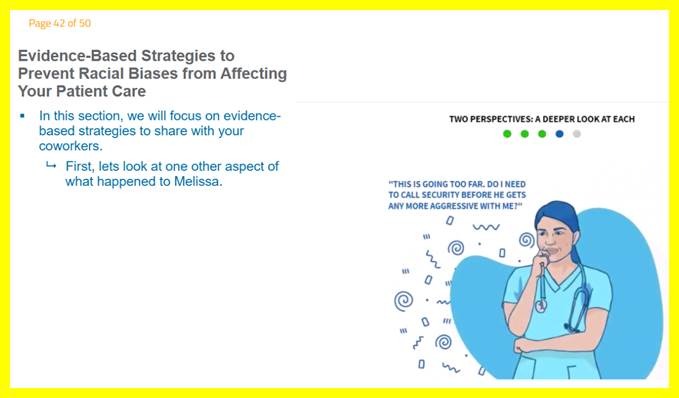
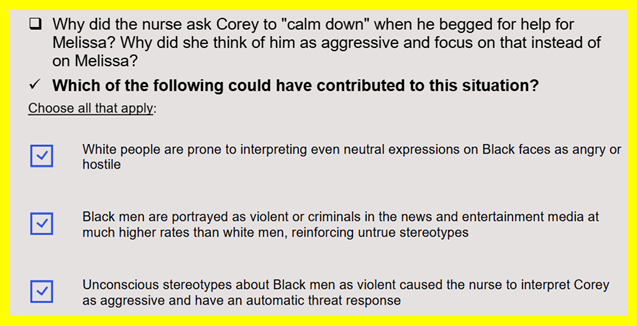
According to the workshop’s agenda, students were then subjected to various DEI-related activities.
These included a video titled “Allegories on Racism,” as well as a quiz on “equity/diversity awareness.”
In sum, it’s clear that MCW is intent on injecting radical identity politics into its curriculum.
This is not the function of medical education, pure and simple. MCW should focus on educating the best possible physicians, not training the next generation of radical activists.