Today, Do No Harm released a new report on racial concordance in medicine entitled “The Return of Segregation.” This report debunks the narrative pushed by medical organizations and political leaders that matching the races of physicians and patients leads to better healthcare outcomes.
“Healthcare and media organizations continue to push racial concordance despite the weight of evidence against it,” said report author and Do No Harm Director of Research Ian Kingsbury. “These groups are playing a dangerous game by putting their politics over scientific evidence and cherry-picking preferred studies to reach their political goals. We hope our report puts to rest the fashionable but dangerous idea of racial segregation in medicine.”
“The research that claims to find evidence of the benefits of racial concordance in healthcare is generally of low quality,” said report co-author and Do No Harm Senior Fellow Jay Greene. “Even the studies that appear in higher-status journals have obvious and severe defects that prevent them from being offered as support for racial concordance. The fact that such low-quality research appears in top journals says more about the politicization of research than it does about racial concordance.”
“We all want to see the elimination of healthcare disparities, but without solid proof that racial concordance would benefit patients we needlessly racialize an aspect of American life and divide American communities,” said Do No Harm Chairman Dr. Stanley Goldfarb. “The same divisive identity politics pushed by supporters of ‘diversity, equity and inclusion’ is being used as the basis for racial concordance.”
Top Takeaways
Of the systematic reviews of racial concordance, four of five show no improvement in healthcare outcomes when segregating patients and doctors based on race.
Racial concordance holds no promise for producing better care or better outcomes. Instead, patient-provider pairings should be determined by convenience, practicality, and expertise.
Efforts to increase the number of doctors from any particular racial group will not result in better patient care. Attempts by medical schools to deprioritize merit and skirt the Supreme Court’s ban on affirmative action would instead jeopardize patient care. Research indicates that strong academic readiness, not racial concordance, predicts clinical performance.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-12-19 17:30:442026-02-11 15:33:41Do No Harm Releases New Report: “Racial Concordance in Medicine: The Return of Segregation”
Three cheers for Oklahoma. On December 13, Governor Kevin Stitt took a major step toward rolling back divisive and discriminatory ideology at public universities, including the state’s two medical schools. So-called “diversity, equity, and inclusion” is now on the retreat in Oklahoma.
Gov. Stitt signed an executive order with multiple necessary reforms. University faculty, staff, students, and applicants are protected from being forced to sign “DEI statements” or other forms of woke loyalty oaths. What’s more, state funds and property can no longer be used toward for woke training or on departments that “grant preferential treatment” based on “race, color, sex, ethnicity, or national origin.”
That’s essentially a ban on DEI departments. But DEI goes well beyond specific departments, which is why the Governor’s order also requires universities to review their overall DEI policies. That will sure bring plenty of disturbing policies to light.
The Governor rightly declared that “diversity is an asset that shouldn’t be abused to advance a political agenda.” He further stated that Oklahoma is now “taking politics out of education and focusing on preparing students for the workforce.”
Yet the President of the University of Oklahoma is trying to defend the indefensible. In a letterresponding to the executive order, he stated “this news evokes deep concern and uncertainty about the future, and in many ways feels like a step backward.” In fact, Oklahoma’s reform is a huge step forward.
The OU President’s letter indicates that state universities and medical schools will surely try to get around this order. They’re obsessed with DEI and determined to continue spreading division and discrimination. DEI initiatives have embedded identity politics into all aspects of university life. The result of this has been to further group-based biases like anti-Semitism. Beyond Oklahoma, universities like Harvard and others are doubling down on DEI. Oklahoma schools likely want to do the same, regardless of state restrictions.
Do No Harm will be watching them closely. We’re grateful to Gov. Stitt for moving Oklahoma’s higher education in the right direction.
https://donoharmmedicine.org/wp-content/uploads/2023/12/shutterstock_192482924-scaled.jpg16362560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-12-19 13:56:152026-02-11 15:33:41Big Win: Oklahoma Bans University DEI Departments
On August 10, 2023, the Detroit News published an article by Do No Harm Senior Fellow and Licensed Marriage and Family Therapist Stephanie Winn on the truth behind “conversion therapy” bans.
The U.S. Supreme Court ruled in June that the use of race-based admissions practices isn’t constitutional in higher education settings, including medical schools. But the Association of American Medical Colleges (AAMC) continues to promote a recruiting tool that aggregates information on medical school applicants who “self-identify as being from groups historically underrepresented in medicine or who are economically disadvantaged.”
The AAMC, which oversees the Medical College Admission Test (MCAT) and cosponsors the accrediting body for all medical schools, appears to be continuing in their efforts to find ways to undermine the Court’s landmark ruling.
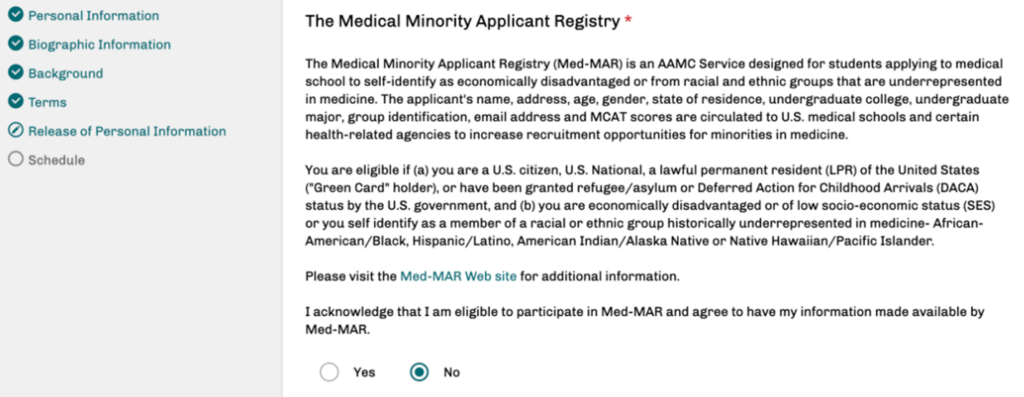
Do No Harm obtained a screenshot from the MCAT registration platform describing the “Medical Minority Applicant Registry” (Med-MAR), which requires the applicant to provide specific information about his or her race and ethnicity. The registrant must opt-in to this service, which AAMC says “enhances admission opportunities for students from groups historically underrepresented in medicine.”
This description has not changed since at least April 2021, which is the first time the program’s webpage was archived.
Figure 1. Screen that candidates see when logging into the AAMC’s MCAT registration website.
“If you choose to participate in Med-MAR, your basic biographical information and your MCAT scores will be distributed to the minority affairs and admission offices of AAMC-member schools and to select health-related agencies whose mission is to increase opportunities for students historically underrepresented in medicine,” AAMC tells applicants from racial and ethnic political identity groups.
They indicate by omission that whites and Asians need not apply:
You are eligible if (a) you are a U.S. citizen, U.S. National, a lawful permanent resident (LPR) of the United States (“Green Card” holder), or have been granted refugee/asylum or Deferred Action for Childhood Arrivals (DACA) status by the U.S. government, and (b) you are economically disadvantaged or of low socio-economic status (SES), or you self-identify as a member of a racial or ethnic group historically underrepresented in medicine–African-American/Black, Hispanic/Latino, American Indian/Alaska Native or Native Hawaiian/Pacific Islander.
Interestingly, the AAMC offers a disclaimer for the Med-MAR system: “Med-MAR serves only as a means of identifying and communicating the availability of applicants from groups who self-identify as underrepresented in medicine and/or as economically disadvantaged. No attempt is made by Med-MAR to advise students where to apply or to influence any admissions decisions.”
As Do No Harm notedin August, AAMC continues to push ways to erode the Court’s ruling.
“Nothing in the Supreme Court decision compels us to deviate from our goal of diversifying the health care workforce,” AAMC CEO David Skorton said during a webinarwith medical school leaders in July.
Strategies promoted by AAMC include:
Holistic review – a term that conceals the word “race” but urges medical schools to subjectively consider the “whole” applicant;
Essays penned by the applicants to evaluate strengths and experiences that might be related to their race; and
The development of strong relationships with undergraduate schools and community groups with a high percentage of racial and ethnic minorities.
Do No Harm has been following AAMC’s plunge into radical Critical Race Theory-inspired DEI practices for some time. And, because of its heavy influence over medical school officials, the organization has taken these institutions along with it.
In November 2022 – prior to the Court’s ruling against affirmative action policies – Do No Harm Chairman Stanley Goldfarb, M.D. sounded the alarm that medical schools seeking accreditation were being coerced into expanding their woke practices.
In a survey of 101 institutions, Goldfarb wrote at the New York Post, AAMC asked schools to respond to 89 questions about whether they employ particular DEI practices.
The Do No Harm chairman revealed the results of AAMC’s “report card”:
All told, more than six out of 10 medical schools scored 80%. The Ohio State University College of Medicine audit shows a score of 93%, making it one of the most woke medical schools in America. Crucially, no institution scored lower than 50% — meaning virtually every medical school is implementing at least half the policies woke activists want.
Goldfarb observed at the time that medical schools have organized and well-funded bureaucracies in place pushing woke ideology on both faculty and students.
“These efforts take away time and money from actual education,” he asserted, adding:
The AAMC is pushing 100% of medical schools to score 100% in each category, and most are trending in that direction. This doesn’t bode well for the future of health care. Medical schools are broadly lowering standards for admissions, faculty and research while devoting a higher share of resources to political lobbying, politicized bureaucracy and public virtue signaling.
In the majority opinion, Chief Justice Roberts noted that implementing “application essays or other means” is not a valid tactic for universities to get to the results they had prior to the decision ending race-based admissions. “In other words,” he continued, “the student must be treated based on his or her experiences as an individual – not on the basis of race.” Workarounds such as these will undoubtedly be successfully challenged. Yet, considering AAMC’s continued use of the Med-MAR applicant registry service for specific racial and ethnic groups, not much has changed in this organization in the wake of the Court’s ruling.
A program at the Ohio University Heritage College of Osteopathic Medicine (OUHCOM) is under investigation by the U.S. Department of Education’s Office for Civil Rights (OCR) for illegal racial discrimination – and the school wasted no time in scrubbing its website of the evidence.
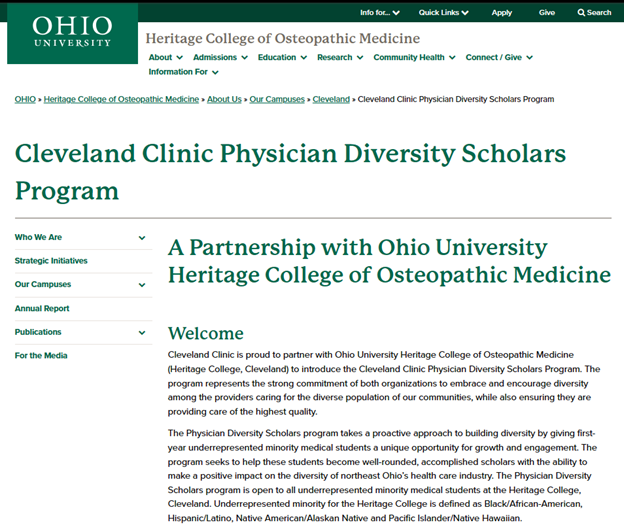
Offered in partnership with the Cleveland Clinic, the Physician Diversity Scholars Program “takes a proactive approach to building diversity” by being “open to all underrepresented minority medical students” at OUHCOM (archived page here). “Underrepresented minority for the Heritage College,” the website stated, “is defined as Black/African-American, Hispanic/Latino, Native American/Alaskan Native and pacific Islander/Native Hawaiian.”
Limiting eligibility to specific racial groups while excluding others violates Title VI of the Civil Rights Act of 1964, which prohibits discrimination on the basis of race.
Figure 1. Cleveland Clinic Physician Diversity Scholars Program at OUHCOM, as seen on May 12, 2023.
The modified webpage now says that the program provides “purposeful and meaningful health care interactions with community populations that are underrepresented in medicine.”
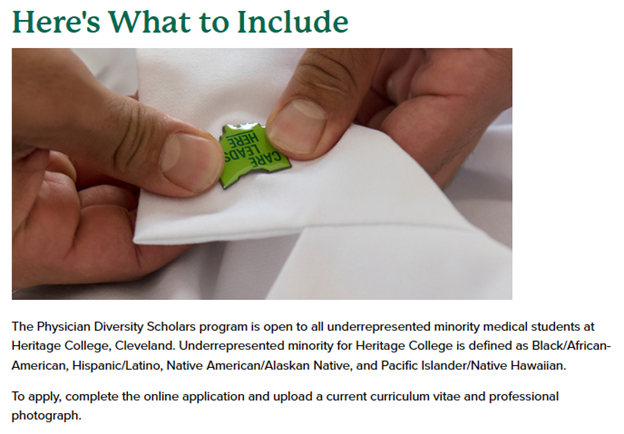
At the time the complaint was filed with the Cleveland OCR, the “How to Apply” page provided further evidence of OUHCOM’s intent to discriminate, reiterating the racial/ethnic groups that were eligible and instructing applicants to include a professional photograph (archived page here).
Figure 2. Application instructions Cleveland Clinic Physician Diversity Scholars Program at OUHCOM, as seen on May 12, 2023.
The cleanup was not as thorough on this page, as it still states, “The Physician Diversity Scholars program is open to all historically underrepresented students in medicine at Heritage College, Cleveland.” However, the specific racial/ethnic categories have been removed in the modified version.
Ohio taxpayers and the lawmakers who represent them must ask the Ohio University Heritage College of Osteopathic Medicine why the school is willing to remove a discriminatory program only after a federal civil rights complaint is filed and an investigation is opened. Do No Harm will be monitoring for full resolution of our complaint.
https://donoharmmedicine.org/wp-content/uploads/2023/10/shutterstock_2167014079-scaled.jpg13502560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-12-15 13:28:072026-02-11 15:33:41Ohio University Heritage College of Osteopathic Medicine Scholars Program Is the Subject of a Federal Civil Rights Investigation
The University of Missouri-Columbia School of Medicine (Mizzou Med) said that it didn’t participate in the Association of American Medical Colleges’ (AAMC) Diversity, Inclusion, Culture, and Equity (DICE) Inventory, but its devotion to all things DEI raise the question of “why not?”
The DICE Inventory is an 89-question survey that 101 North American medical schools participated in during 2022. Institutions voluntarily submitted their yes/no answers to AAMC, indicating whether or not they engage in specific DEI-related initiatives, programs, or practices. Last year, Do No Harm submitted a Freedom of Information Act (FOIA) request to Mizzou Med for the school’s DICE Inventory response, but the Custodian of Records for the University of Missouri System told us, “I am informed there is no document responsive to your request.”
A follow-up query confirmed that Laura Henderson Kelley MD, MPH advised that no such document exists. Board certified in internal medicine and pediatrics, Dr. Henderson Kelley carries the title of “Associate Dean for Diversity, Inclusion, Culture, and Equity (DICE),” and leads the school’s Office of Diversity and Inclusion (ODI).
Yet Mizzou Med follows the AAMC on other DEI-related concepts.
The Equity, Diversity, and Inclusion Cluster document, received by Dr. Henderson Kelley in March 2022, further illustrates Mizzou Med’s dedication to the AAMC’s guidance on DEI. The document, supported by Dr. David Acosta, AAMC’s Chief Diversity and Inclusion Officer, provides direction “to assist you with the DEI work at your institutions.” The Cluster document includes “three portfolios” of Equity and Social Accountability (ESA); Workforce Diversity; and Organizational Inclusion and Development. For example, the Cluster document notes that the ESA Portfolio will help medical schools to become “anti-racist leaders who acknowledge and understand systemic racial inequities,” as well as adopting policies “that promote racial justice and equity.”
Figure 1. Examples of initiatives in the ESA Portfolio of the AAMC Cluster document.
As reported in April, Mizzou Med provided its Class of 2024 orientees with the Common Read program “to facilitate meaningful conversations around health inequities and social injustice early in medical school education.” This aligns with the ESA Portfolio’s aims to “develop an emerging generation of physicians with an equity mindset” and “encourage the inclusion of anti-racism” in the curriculum. This conviction was readily apparent during the 2023 legislative season when 150 students at the medical school demanded that state lawmakers “protect our school’s right to require DEI education.”
The Class of 2024 was also informed by Steven Zweig MD, dean of medical school, that their newly received white coats symbolize “a commitment to fighting racism in medicine.”
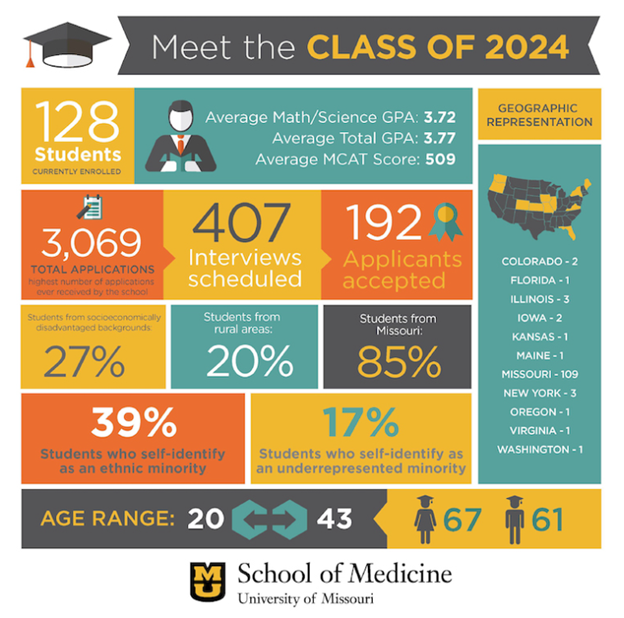
The Mizzou Med Class of 2024 is also aligned with the AAMC’s Workforce Diversity Portfolio aim of increasing the numbers of students “who are underrepresented in the health professions,” and prepared an infographic to illustrate it. AAMC recommends holding career fairs and workshops for “diversifying the next generation of doctors” or participating in the “Action Collaborative for Black Men in Medicine” to achieve that metric. The university has long shown that it fosters discrimination on the basis of race with scholarships it offers within the School of Medicine. The Office for Civil Rights is currently investigating Mizzou Med for ten scholarships that violate Title VI of the Civil Rights Act of 1964, which prohibits such discrimination.
Figure 2. Mizzou Med Class of 2024 enrollment information.
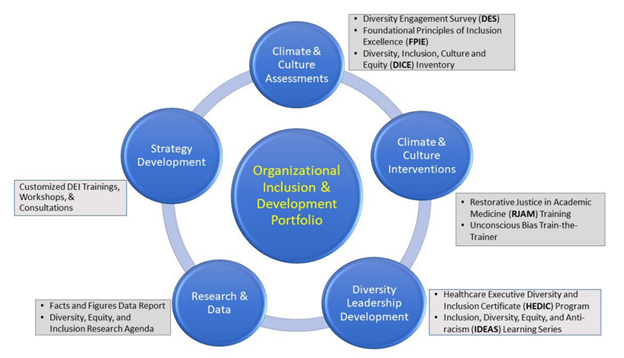
But the Cluster document’s most concerning recommendations come from the Organizational Inclusion and Development Portfolio, as it recommends actions for “equity-minded medical schools” that infuse the DEI agenda into every corner of their operations.
Figure 3. AAMC’s Organizational Inclusion and Development Portfolio.
A new six-session faculty course titled “Addressing and Reducing Cultural Bias in Medicine” was recently sponsored by Mizzou Med, featuring instruction on “medical racism” and “privilege, implicit bias, and microaggressions.” The topics in this course demonstrate how the school aligns with initiatives recommended by the AAMC in the Cluster document, such as the Inclusion, Diversity, Equity, and Anti-racism (IDEAs) Learning Series and the Restorative Justice in Academic Medicine (RJAM) training program.
These concepts do not reflect what it means to receive an education in the art and science of medicine. Do No Harm calls on Mizzou Med to return its focus to the patient-based training it claims to offer, which is in the best interests of the individuals its graduates who will one day be responsible for diagnosing and healing.
https://donoharmmedicine.org/wp-content/uploads/2023/12/shutterstock_380551900-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-12-13 14:31:202026-02-11 15:33:41Mizzou Med Claims “No DICE,” But Its Actions Suggest They Are Still Fully On Board With DEI
The Joint Commission (TJC) is familiar to healthcare professionals as the entity that has them scrambling to prepare in the days and weeks prior to an accreditation survey of their facilities. The patient safety realm is a large part of TJC’s mission to ensure healthcare organizations “excel in providing safe and effective care of the highest quality and value” for the public. But there’s a new National Patient Safety Goal (NPSG) that claims identifying patients by race and ethnicity – rather than as individuals – will make “safety” a priority.
Based on an element of the Leadership chapter of TJC’s accreditation standards (LD.04.03.08) “which addresses healthcare disparities as a quality and safety priority,” NPSG 16 took effect July 1, says the TJC’s website (archived link). Although the accreditation requirements aren’t changing, TJC adds, “the change is being made to increase the focus on improving healthcare equity versus reducing healthcare disparities.” This is outside the usual tone of the NPSGs over the past twenty years, which traditionally focus on true patient safety issues such as improving staff communication and using medications safely. NPSG.16.01.01 states:
Improving healthcare equity is a quality and patient safety priority. For example, healthcare disparities in the patient population are identified and a written plan describes ways to improve healthcare equity.
To achieve this NPSG (which is being extended into 2024), hospitals and other healthcare facilities seeking TJC accreditation, including ambulatory and behavioral healthcare organizations, are required to:
Identify an individual to lead activities to improve healthcare equity.
Assess patients’ health-related social needs.
Analyze quality and safety data to identify disparities.
Develop an action plan to improve healthcare equity.
Act when the organization does not meet the goals in its action plan.
Inform key stakeholders about progress to improve healthcare equity.
“Organizations need established leaders and standardized structures and processes in place to detect and address healthcare disparities,” TJC says in one of its R3 Report (Requirement, Rationale, Reference) documents, emphasizing again that a focus on a patient’s racial and ethnic identity is on par with essential safety concerns.
“These efforts should be fully integrated with existing quality improvement activities within the organization like other priority issues such as infection prevention and control, antibiotic stewardship, and workplace violence,” TJC states.
TJC’s requirement, however, of the identification of a “leader” of an organization’s “healthcare equity” activities, along with “standardized structures and processes” in order to “detect and address healthcare disparities” sets up another bureaucracy focused on political identity groups, rather than individualized patient care.
The commission appears to try to refute this criticism with the claim it will be focusing on “health-related social needs (HRSNs)” of patients, rather than the population-centered “social determinants of health (SDOH).”
HRSNs, TJC argues, are a “proximate cause of poor health outcomes for individual patients.”
“Understanding individual patients’ HRSNs can be critical for designing practical, patient-centered care plans,” the commission continues its argument, using the examples of “a care plan for tight control of diabetes may be unsafe for someone with food insecurity, and outpatient radiation therapy may be impractical for someone who lacks reliable transportation to treatment.”
All healthcare organizations, however, have social work services already in place to assist patients with special needs to obtain necessary medical treatments. Setting up and funding a new bureaucracy based on DEI ideology and activism seems more politically expedient than required for “safe and effective care of the highest quality and value.” Such mandates impose even more burdens on healthcare providers to address patient socioeconomic issues, rather than focus on delivering quality medical care.
Hospitals and other healthcare organizations seeking Joint Commission accreditation are invited to use the “Health Care Equity Accreditation Resource Center” in order to meet the new standards. But even with such a robust collection of resources, it is difficult to determine exactly how TJC defines health care equity. “And although health care equity is often viewed through a social justice lens,” TJC says, “we understand it to be first and foremost a quality-of-care problem.” Before “sustainable improvement” in health outcomes for minorities can be attained, institutions must start by “understanding the root causes and implementing targeted standards of care,” TJC claims.
Do No Harm Chairman Stanley Goldfarb, M.D. recently pointed out how the evidence to support racial inequity as the root cause of health disparities simply isn’t out there.
“The research establishment studying racial disparities in healthcare has a big problem,” Goldfarb stated in a piece in May at City Journal. Researchers have made “a concerted effort to ignore any literature” that contradicts their belief that differences in health outcomes are due to race-based factors.
The former associate dean of the University of Pennsylvania Perelman School of Medicine asserted that “the largest study of racial concordance, which included 56,000 patients, failed to show a benefit.” Yet other publications in the literature that provide “useful information about actual healthcare outcomes” have been largely ignored.
With NPSG 16, TJC is disregarding the difference between eliminating health disparities and producing health equity. Efforts aimed at removing health disparities include implementation of programs and processes with the goal of improving the delivery of healthcare for everyone. However, measures to create health equity are focused only on patient groups that meet certain racial identity criteria, while doing nothing to innovate healthcare delivery for groups of patients who do not fall into those categories. Regardless of the latest labels used to describe it, the promotion of “health equity” is a discriminatory practice.
The Joint Commission once used the best available scientific evidence to set its standards for improving patient safety and quality of care. Considering its level of influence over the delivery of services across the continuum of patient care in more than 22,000 organizations, TJC must return to being guided by facts, not ideology, as a means to achieve patient safety goals.
https://donoharmmedicine.org/wp-content/uploads/2023/12/shutterstock_1021932094-scaled.jpg15202560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-12-12 12:37:412026-02-11 15:33:41The Joint Commission Requires ‘Safety Goal’ of DEI’s ‘Healthcare Equity’ for Organizations Seeking Accreditation
The Association of American Medical Colleges’ (AAMC) powerful dual role in overseeing the Medical College Admission Test (MCAT) and cosponsoring the accrediting body for all medical education programs in the U.S. puts pressure on the schools to adopt its diversity, equity, and inclusion (DEI) agenda. Elite universities employ DEI proponents to embed this organization’s ideologies into all aspects of their programs, and the University of Missouri-Columbia School of Medicine (Mizzou Med) is no exception.
Freedom of Information Act (FOIA) documents obtained by Do No Harm show how Robin Clay, M.Ed., the manager for DEI initiatives at Mizzou Med, pushed out highly politicized AAMC events and trainings throughout 2022. According to his MU bio, “Robin is a passionate student advocate who is excited to train future, patient-centered, and socially conscious physicians.”
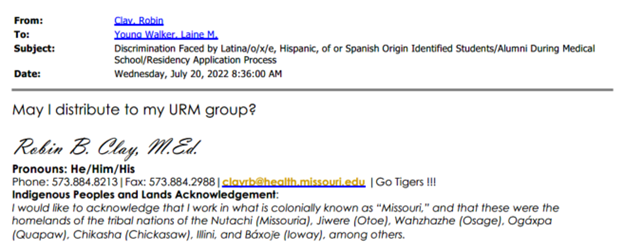
For example, Clay sought permission from Dr. Laine Walker, Associate Dean for Student Programs, to forward a message from an AAMC listserv regarding Discrimination Faced by Latina/o/x/e, Hispanic, of or [sic] Spanish Origin Identified Students/Alumni During Medical School/Residency Application Process. “May I distribute to my URM [underrepresented in medicine] group?” he asked Walker. AAMC was informing DEI officials of an upcoming needs assessment of “LHS+ medical students and alumni” to produce a report that would inform “best practices to reduce the burden of discrimination.”
Figure 1. July 20, 2022 email from Robin Clay (DEI manager) obtained via FOIA from Mizzou Med.
Additionally, on September 1, Clay received an AAMC notice of an upcoming “GSA [Group on Student Affairs] Working Group on Medical Student Wellbeing Fall Community Call Series” event, which said that “the wellbeing of medical students depends on their learning environment, school structures and processes, and institutional culture.” “In this interactive session, presenters will discuss structural and systematic issues (p/f grading, asynchronous learning) and curricula that impact wellbeing,” the statement continues. “Participants will leave with practical tools to design and implement curricula using different teaching modalities at their home institution and to advocate for systemic and structural initiatives to support medical student wellbeing.” What this translates into is the lowering of academic standards in the name of perceived systemic inequities.
On the following day, Clay forwarded to his colleagues AAMC’s promotion of a CGSA “Community Call on Signaling and the Supplemental Application.” “This is a good community call that may help better advise our 4th year students,” Clay wrote. “I wonder if there are ways we can use this to improve diverse residents in our programs,” he added.
On November 30, 2021, he forwarded an announcement for a highly controversial webinar to a University of Missouri staff member asking, “How can we send this to the president…” The January 2022 webinar, titled Socially Accountable Admissions: Using a different lens to evaluate medical school applicants and promote workforce diversity, was presented by AAMC in cooperation with the UC Davis medical school.
As Do No Harm reported in June 2023, the presenters provided information to admissions officials, including statements that MCAT scores are of limited value and their use leads to “overrepresentation” of Asian physicians.
Mizzou Med currently demonstrates its ongoing alignment with AAMC’s DEI mission by designating “societal and cultural issues” as a component of the medical education program, establishing minimal academic standards for admission, and maintaining a robust DEI office.
Do No Harm will be monitoring the actions of Mizzou Med for their commitment to DEI instead of medical education in the months and years to come.
https://donoharmmedicine.org/wp-content/uploads/2023/12/shutterstock_1497815498-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-12-11 21:28:242026-02-11 15:33:41University of Missouri Medical School Official Propagates the AAMC’s DEI Mission
Pensacola, FL – Do No Harm, a prominent national nonprofit committed to safeguarding healthcare from radical and divisive ideology, filed a lawsuit against the unlawful and discriminatory leadership program offered by Vituity in which there are leadership incentives exclusively for one race.
Vituity, a medical staffing agency, proudly promoted the “Bridge to Brilliance Incentive Program” which is solely offered to black physicians along with a sign-on bonus of up to $100,000. This program is a direct violation of numerous federal laws, including the Affordable Care Act, section 1557 which prohibits racial discrimination in “any health program or activity, any part of which is receiving federal assistance.”
“Black patients want the best doctors and the best medical care – not doctors that are racially concordant. Vituity’s Bridge to Brilliance Program, which offers physicians hiring opportunities and sign on bonuses on the basis of race is abhorrent and rightfully illegal. Medical staffing agencies like Vituity are given the important responsibility of offering medical positions to the most qualified medical professionals. Like all aspects of healthcare, patient safety and patient concerns should be primary, not the skin color or the racial makeup of their physician. Medical professionals should be hired on merit alone.” Dr. Stanley Goldfarb, board chair of Do No Harm.
Do No Harm is asking the Court to enter judgment in its favor against Vituity by:
Providing a declaratory judgment that Vituity’s “Bridge to Brilliance” incentive program violates section 1981 and the ACA;
Issuing a temporary restraining order and preliminary injunction barring Vituity from closing the application period, selecting and offering applicants positions within in the program, or enforcing racially discriminatory criteria before the lawsuit is resolved;
Issuing a permanent injunction barring Vituity from enforcing its racially discriminatory eligibility criteria for the program.
The case is Do No Harm v Vituity (CEP America LLC.) and was filed in The United States District Court for the Northern District of Florida Pensacola Division. Find additional information here: Do No Harm v. Vituity
###
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. With more than 5,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and in 14 countries, DNH has achieved more than 4,900 media hits in top-tier publications and garnered widespread attention through numerous broadcast news appearances.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200rededge-rachelhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngrededge-rachel2023-12-11 14:26:122026-02-11 15:33:41Do No Harm Challenges Vituity’s (CEP AMERICA LLC.) Racially Discriminatory Leadership Program
The “host committee” of Family Medicine Education Consortium, Inc.’s (FMEC) 2023 annual meeting program set the tone for its conference by announcing the practice of family medicine is now “anchored in the biopsychosocial model of care that promotes high quality, equitable care” – woke-speak for Critical Race Theory (CRT)-inspired diversity, equity, and inclusion (DEI) ideology.
“Through the telescopes that we use in family medicine, we focus on individuals and their health conditions,” the host committee continued, but then explained its odd view that the medical care a patient requires will vary according to that patient’s social needs.
“We change lenses to see our patients as they need us to, interpreting health care needs in the context of their resources and communities in which they live,” the committee stated.
Do No Harm obtained documents and screenshots related to the FMEC meeting held October 13-15 in Providence, Rhode Island.
One lecture discussion during the meeting was advertised in print to conference attendees (see page 42 of the program) with a key misspelling in the title – which apparently no one picked up prior to publication.
The description of the lecture, delivered by Andria Matthews, M.D. and Gian Grant-McGarvey, M.D., for “Infusing Anti-Rascist [sic] Objectives into Medical School Curriculum” taught attendees how to incorporate CRT tenets into medical school curricula:
As part of the Academic Family Medicine Antiracism Learning Collaborative of the Society of Teachers of Family Medicine (STFM), Dr. Matthews, Dr. Grant-McGarvey and the UCONN School of Medicine Student Diversity, Equity and Inclusion Committee have worked collaboratively to incorporate anti-racist objectives into the UCONN Medical School curriculum and evaluate student and faculty comfort with learning and teaching anti-racist content. Dr. Matthews and Dr. Grant-McGarvey will share learnings from the project, including how they developed anti-racist content, incorporated medical student feedback, supported faculty in increasing comfort with discussions about race and racism and evaluated progress in these areas.
Figure 1. Session offered at the 2023 FMEC Conference (October 15, 2023).
Do No Harm obtained additional screenshots of descriptions of other FMEC meeting workshops, including “Improving DEI in Residency Recruitment: A Scoping Review,” a presentation that championed the “health equity” narrative that claims “systemic racism” and “oppression” prevent minority individuals from obtaining access to adequate health care. According to the radical dogma, if there are more healthcare providers from “marginalized” identity groups, more patients from these same minority groups will obtain higher quality health care.
“Many persons in the United States do not see their racial, ethnic, or gender identity reflected in the physicians who care for them,” the session description read and then expressed disappointment that “[d]espite increased interest in diversifying the US physician workforce, recruiting diverse residency classes remains challenging for many programs.”
The workshop featured results of a “scoping review to understand the current evidence base” regarding the incorporation of DEI practices into residency program application processes – all to ensure that future practicing doctors are members of certain racial, ethnic, and sexuality political identities.
FMEC’s promotion of radical gender ideology was also evident in its conference workshop titled “Incorporating Lactation into Family Medicine Residency Curriculum.”
Swapping out the biologically-based term “breastfeeding” for the gender-neutral “chestfeeding,” FMEC’s description lauded “the profound benefits of chestfeeding,” and advocated for “having a lactation curriculum in Family Medicine residency” in order to enhance pediatric and maternal health curricula.
Figure 2. Sessions offered at the 2023 FMEC Conference (October 14, 2023).
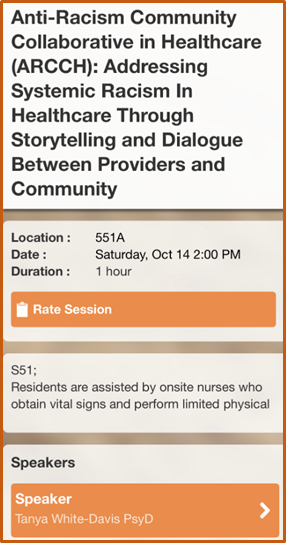
Yet another FMEC workshop was titled “Anti-Racism Community Collaborative in Healthcare (ARCCH): Addressing Systemic Racism in Healthcare Through Storytelling and Dialogue Between Providers and Community.”
Figure 3. Session offered at the 2023 FMEC Conference (October 14, 2023).
Documents from the FMEC meeting also show Kristina Johnson, M.D. and Stephanie Miller, M.D. of Forbes Family Medicine Residency Program presented a demonstration of a “lecture-discussion” used for interns during orientation of the CRT-inspired tenet of “racial health disparities,” which the presenters defined as “a preventable difference in health between racial groups.”
Johnson and Miller, however, did not stop at racial disparities. They went on to claim that “gender, religion, socioeconomic status, sexual orientation, and physical disability” can also be tied to health disparities.
The presenters provided a quote from Critical Race Theory: An Introduction, by Richard Delgado and Jean Stefancic, that claims race is not a “biological or genetic reality,” but a social construct.
The materials indicate the purpose of the presentation was to encourage doctors to become both social workers and political activists for their patients’ social causes.
Figure 4. From “Hesitant to Teach About Racial Health Disparities? Start Here!” by Johnson and Miller at FMEC 2023.
“A person’s health is heavily influenced by the social determinants of health – which occur outside of the health care setting,” the document read. “Our goal is to empower family physicians to advocate for changes outside of the clinical space to improve the health of their communities.”
While CRT tenets are currently being taught in U.S. medical schools, the fact is there is no evidence to support the claim the so-called “social determinants of health” (SDoH) are the causes of health disparities.
In a piece at City Journal in September, Do No Harm Chairman Stanley Goldfarb, M.D. observed that the central message of a 2017 report on the subject from the National Academy of Medicine was: “no one should attribute any health-care disparities to individuals’ self-determined actions,” and that it’s time to reject the “decontextualized, biomedical framework.”
The SDoH trend in medicine is already embedded in medical school curricula, but “activists want to go further,” Goldfarb wrote, asserting, however, such a vision of doctors as social workers and political activists is “profoundly flawed” and “will only lead to further degradation of our health-care system.”
“Worst of all, it will not do anything to improve the well-being of patients or correct disparities in health outcomes,” he added. “In fact, it is far more likely to worsen patient suffering, since patients will increasingly deal with doctors trained to be political activists instead of true medical professionals.”
https://donoharmmedicine.org/wp-content/uploads/2023/12/shutterstock_1932378590-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-12-08 14:33:122026-02-11 15:33:41Family Medicine Education Consortium ‘Anchored’ in Radical Critical Race Theory
Every month, we receive queries from members and concerned citizens who want to know where to find a college or university that has not succumbed to the infiltration of politicized ideologies.
A great place to start is the interactive map on our homepage, where you can choose a state and see the materials we have gathered on that state’s medical schools and the actions they are taking to perpetuate the DEI agenda. But sometimes there are specific topics that need to be individually highlighted.
Do No Harm has collected information on public and private institutions of higher education that have attempted to place conditions on student admissions or on the hiring, retention, or promotion of faculty members. We have also found instances in which applicants or faculty members are required to make some type of statement or pledge of support to politicized ideologies like diversity, equity, and inclusion (DEI), as seen in posted job descriptions.
It is important to note that the provisions of the Freedom of Information Act (FOIA) limit our ability to request information only from public universities. The document below reflects publicly available information or materials that have been voluntarily provided to us by sources and demonstrates the incidents we have received to date. One must not assume that the institutions listed in the document are the only ones engaging in this type of activity. To inform us of similar incidents you are observing, please contact us via our secure online portal.
Read the full resource by downloading with the link below.
https://donoharmmedicine.org/wp-content/uploads/2023/04/DNH_mocks_contentimages_Resource.png6751200Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-12-07 19:09:442026-02-11 15:33:41RESOURCE: Public and private medical education programs with DEI initiatives for students or faculty
Another medical school has been caught discriminating – and forced to stop.
After Do No Harm filed a federal civil rights complaint for alleged violations of Title VI and Title IX, the University of Colorado’s Anschutz Medical Campus ditched its requirements for three “diversity” scholarships that restricted eligibility on the basis of race, sexual orientation, or gender identity. This is a victory for merit and protecting the civil rights of all students over the widespread woke ideology that has infected US medical schools.
The three “diversity” scholarships could hardly have been more blatantly discriminatory:
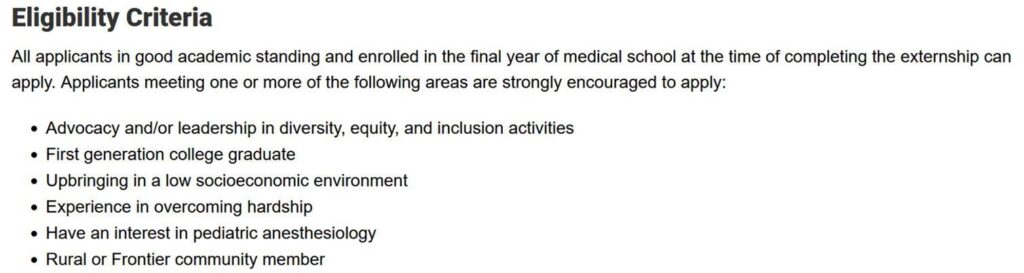
The first scholarship, for anesthesiology students, was only eligible to “African American, American Indian, Alaskan Native, Hispanic/Latino, Pacific Islander, and/or LGBTQIA” applicants.
The secondscholarship, for anesthesiology assistants, was only eligible to “African American, Hispanic/Latino, Pacific Islander, Native American/Alaska native, [and/or] Vietnamese” applicants.
The finalscholarship, for surgical students, was only eligible to “African American, American Indian, Alaskan Native, Hispanic/Latino, Pacific Islander, and/or LGBTQ” applicants.
Do No Harm filed a federal civil rights complaint with the U.S. Department of Education’s Office for Civil Rights in June, pointing out that such discrimination violates federal civil rights laws that prohibit discrimination on the basis of race, color, national origin, sexual orientation or gender identity. The Office for Civil Rights has now closed the case after working with the University of Colorado to eliminate its illegal restrictions. This is another troubling example of a university that was either inexcusably unaware of its legal obligation to actively enforce federal civil rights or unacceptably unconcerned about violating the civil rights of certain medical students based on their race or sex.
Figure 1. Eligibility criteria for the Medical Externship Diversity Scholarship as seen on June 4, 2023.Figure 2. Current eligibility criteria for the Medical Externship Diversity Scholarship.
In the wake of the Supreme Court’s recent decision to end affirmative action for college admissions, medical schools should be on notice that no form of race-based discrimination is allowed whether it’s for admissions, financial aid, or academic programs. They need to understand that race-based and sex-based discrimination is still unlawful even if it advantages the “right” race or sex for the “right” reasons.
Do No Harm will keep fighting against illegal discrimination at medical schools. And as the University of Colorado just learned, Do No Harm knows how to win. But the real winners are the most qualified applicants to medical school and the patients they will eventually treat.
https://donoharmmedicine.org/wp-content/uploads/2023/12/shutterstock_759889465-scaled.jpg17092560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-12-05 14:10:232026-02-11 15:33:41Big Win: University of Colorado Ditches Its Illegal Discrimination
Radical ideology is arguably even more advanced in Canadian health care than it is in the United States. The latest proof: The Royal College of Physicians and Surgeons may force medical students to learn more about “anti-racism” than actual medicine. Canadian health care is on the fast track to racial division and discrimination.
The Royal College’s proposal is astounding. It concerns CanMEDS, the framework for physician training that will be updated in 2025. The Royal College’s anti-racism working groups states it wants “a new model of CanMEDS” that “would seek to centre values such as anti-oppression, anti-racism and social justice, rather than medical expertise.” [Emphases added.] In other words, treating patients’ medical conditions is less important than treating them as oppressors or victims.
Do No Harm senior fellow Dr. Roy Eappen, a practicing endocrinologist in Montreal, has made clear the stakes:
I am quite concerned by the new DEI proposals of the Royal College. Patients expect competence from their physicians in diagnoses and treatment. They expect compassion and a thorough knowledge of their field and the emerging knowledge in their fields. The Royal College has a long tradition of excellence in teaching and upholding the profession. The new proposals seem to abrogate that tradition of excellence. We do not do our patients or our profession any favours by taking our eyes off the real goal of patient care and wellness.
Dr. Eappen is not alone. We’ve heard from many Canadian medical professionals who are deeply concerned about the coming corruption of their country’s health care. If that describes you, please consider signing the following statement from Do No Harm:
“Medical expertise is the only acceptable foundation of medicine. The Royal College of Physicians and Surgeons should immediately reject any proposal to replace or water down medical training with political ideology, including anti-oppression, anti-racism, and social justice. The health of every Canadian hangs in the balance.”
If you’re a Canadian medical professional who would like to sign this statement, please see below.
And please consider submitting an official comment on the CanMEDS proposal. Responses are due by December 31, 2023. Canadian patients are counting on you.
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_126213080-scaled.jpg17142560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-12-04 20:07:322026-02-11 15:33:41Stop Canada’s Plan To Corrupt Medicine
Mark J. Perry, Ph.D. is a senior fellow at Do No Harm, and he’s been busy.
Mark joined us a little more than a year ago. Since then, he’s filed more than 110 complaints with the Department of Education’s Office for Civil Rights (OCR) against U.S. medical schools for race-based and sex-based discrimination.
Of those complaints, 38 have been opened so far for investigation, and most have been resolved in our favor. And that’s just since Mark joined us—in total, he’s filed nearly 900 federal civil rights complaints over the last five years for more than 2,000 violations of Title VI (race-based discrimination) and Title IX (sex-based discrimination) at more than 800 colleges and universities. “There is no ‘good’ form of discrimination, regardless of your intentions. It’s all bad and illegal when it violates the law,” Mark says.
Almost every U.S. medical school has at least one scholarship, fellowship, clerkship, award, internship, special preference, or academic program that violates federal civil rights laws.
Most of the illegal discrimination taking place in medical schools involves preferences for students who are considered to be Underrepresented in Medicine (URiM), which typically includes students who are Black, Hispanic or Native American—and excludes white, Asian, Middle Eastern, and North African students.
Mark first learned of URiM programs after getting connected with Do No Harm in 2022 and has led our efforts to challenge these illegal programs ever since.
He recently filed a Title VI complaint against two illegal URiM programs at the University of Nebraska Medical Center—a scholarship and a clerkship. In response to the ensuing OCR investigation, both programs were suspended. The school has since pledged that if both programs resume in the future, they will be open to all applicants, regardless of race.
“If you’re going to provide any type of financial aid for students, it should be open to all students regardless of race, color, national origin, sex, or sexual orientation. Because that’s the law,” Mark explains.
Mark Perry, Do No Harm senior fellow.
Anybody can file a complaint with the Office for Civil Rights. It’s not a lawsuit, and you do not need a lawyer or a complainant with legal standing. And doing so has a real impact.
When the Chronicle of Higher Education contacted 20 of the colleges and universities that entered into formal resolutions with OCR in response to Mark’s complaints, a few of them already reported admitting applicants who would have been otherwise excluded.
Perhaps the most impressive part of Mark’s impact is that he’s not a lawyer. And he had no prior background in civil rights.
When Mark filed his first complaint, he was just an economics professor at the University of Michigan who saw blatant sex discrimination happening at a nearby school, and he had the courage to legally challenge Michigan State University’s women-only lounge.
The more he paid attention, the more he recognized that race and gender discrimination had become a widespread problem across higher education. “My goal is to force colleges and universities to protect the federally guaranteed civil rights of all students, staff, and faculty on their campuses … and end the inexcusable double standard in higher education for the selective enforcement of Title VI and Title IX,” Marktold the Daily Caller. “Simply put, Title VI and Title IX are for all.”
Mark is an inspiring example of how each one of us has the potential to make a difference, and to right a wrong in the world when we see one. Thanks to him, hundreds of educational and professional programs, scholarships, fellowships, awards, student lounges, and other educational opportunities are now accessible to everyone, equally.
Mark didn’t have to speak up. But he did. And he’s making a big difference.
https://donoharmmedicine.org/wp-content/uploads/2023/01/shutterstock_1191331912-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-12-04 12:00:002026-02-11 15:33:41Meet Dr. Mark J. Perry, civil rights advocate
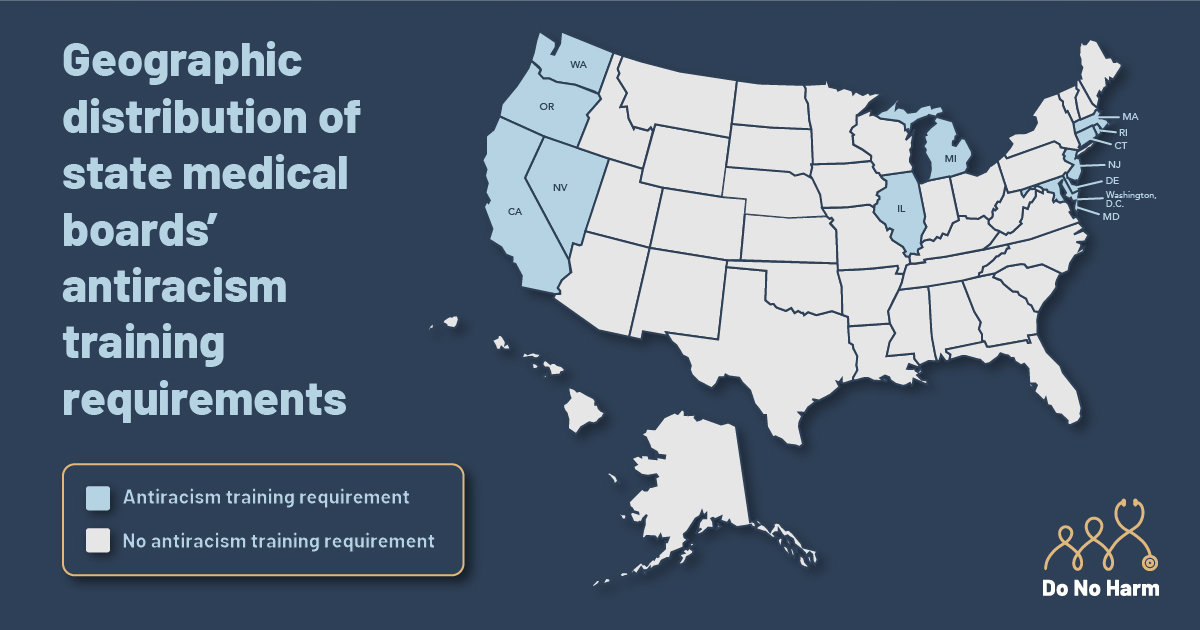
Is your state indoctrinating physicians with extreme racial ideology? The Annals of Internal Medicine has helpfully published a list of states where the answer is yes. Specifically, these states mandate that physicians take “anti-racism” courses as a condition of licensing and/or licensing renewal. Such training divides people by skin color and paves the way for racial discrimination.
The list of states is long and clustered on the coasts, with a few exceptions. On the East Coast, it includes Maryland, Delaware, New Jersey, Rhode Island, Connecticut, Massachusetts, and Washington, D.C. On the West Coast, the list is California, Oregon, Washington, and Nevada. Illinois and Michigan round out the list in the middle of the country.
Adapted from “U.S. State Medical Boards’ Antiracism Education Requirements for Physicians” figure in Annals of Internal Medicine, November 21, 2023 (doi:10.7326/M23-1476).
The Annals of Internal Medicine thinks these mandates are praiseworthy. In publishing the list, it accuses physicians of playing “a key role in perpetrating racial health disparities … including biased clinical decision making and verbal and nonverbal communication.” The mandates are supposed to help physicians realize they’re racist by subjecting them to continuing medical education courses.
But there’s no evidence that such training improves patient outcomes. The accusation behind the training is also insulting. Physicians strive to treat every patient equally, giving them the best possible care regardless of race. While health disparities exist, they reflect a host of other factors, including patient lifestyle choices and other issues — not physician bias.
What’s worse, the training is dangerous, and may even lead to worse patient outcomes. By indoctrinating physicians in the lie that they’re racist, states are encouraging actual racism. “Anti-racism,” according to its most prominent advocate, Ibram X. Kendi, is built on the idea that racial discrimination is essential and even praiseworthy, since it’s supposed to right past wrongs. Yet racial discrimination is always unacceptable, especially in medicine where lives are on the line.
The states with anti-racism training mandates should be ashamed. Better, they should immediately repeal these laws. Do No Harm is already suing California over its mandate, but these unjust policies need to be written out of the law everywhere they exist. Patient health depends on it.
https://donoharmmedicine.org/wp-content/uploads/2023/03/shutterstock_1464629345-scaled.jpg17062560supporthttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngsupport2023-12-01 19:54:112026-02-11 15:33:41These States Force Doctors To Take “Anti-Racist” Training
The University of Michigan Medical School (Michigan Med) has been heavily engaged in diversity, equity, and inclusion (DEI) ideology, spending taxpayer dollars on training that reinforces the claim that medicine is an inherently racist field and that “health equity” requires medical schools to turn out doctors of diverse races and ethnicities through race-based admissions practices.
Documents obtained by Do No Harm via the Freedom of Information Act (FOIA) contained invoices from January 1, 2021 through July 2023, in which the name of the company or the description of services provided included the keywords racial, equity, inclusion, diversity, DEI, diverse, bias, multicultural, human-centric, belonging, and antiracism.
The school engaged in numerous DEI-related training sessions during the period covered by the FOIA documents, paying various speakers for lectures on topics intended to advance an ideological narrative in the field of medicine.
In November 2021, for example, Beverly Griffea Ph.D., president of Mott Community College (MCC), gave a keynote titled, “The Most Important Investment You Will Make” during a symposium focused on “Building Capacity, Building Partnerships: Advancing Health Equity.” She was paid an honorarium of $1,000 by the Michigan Institute for Clinical & Health Research (MICHR) for this presentation. Dr. Griffea hosts a “Diversity, Equity, and Inclusion monthly event” at MCC titled Telling Our Stories, and has stated that MCC’s policies “recognized that diversity, equity, and inclusion are essential to our mission.”
The documents show that, in October 2021 and later in February 2022, the school hired consultant Latisha Cunningham of Leadership and Diversity Consulting (LDC) for a virtual presentation of “Microaggressions: A Deep Dive,” Sessions #1 and #2, billed at $633.33 each. LDC offers this and other workshops, including “dialogues on topics such as race, power and privilege” and “political ideology and expression.”
Sierra Carter, Ph.D., associate professor of psychology at Georgia State University, was paid $500 for a lecture titled “Racial Trauma and Racial Health Disparities among Black American Populations: Examining Pathways to Healing, Collective Action, & Liberation.” Dr. Carter’s research focuses on “racial Health Disparities and the promotion of health equity.” Rosie Alegado of the University of Hawaii is a researcher in biological oceanography, but was paid $300 for services described as a “DEI seminar speaker.”
The documents also contained invoices totaling at least $660 paid to various individuals who provided “expert perspectives on gender-affirming care and gender diverse challenges.”
Medical schools such as Michigan Med are spending precious time and taxpayer funds on training future doctors in radical CRT ideology – when those resources should be used for turning out competent physicians who can identify and treat medical illnesses and disease.
“Can your doctor cure poverty? How about homelessness? Food insecurity?” asked Do No Harm Chairman Stanley Goldfarb, M.D., in a piece at City Journal in September.
Goldfarb answered his own questions:
No. Doctors are trained to treat medical conditions, helping patients lead healthier, happier, longer lives. Yet the medical elite think the answer is “yes.” For years, health disparities between white and minority communities have been attributed to the so-called social determinants of health (SDH), which include the effects of poverty on communities, the residue of historic discrimination, and purported ongoing discriminatory practices in health care.
The recommendation that physicians find solutions for their patients’ social problems is “absurd,” asserts Goldfarb, adding that such a goal “will only lead to further degradation of our health-care system.”
“Worst of all, it will not do anything to improve the well-being of patients or correct disparities in health outcomes,” he wrote. “In fact, it is far more likely to worsen patient suffering, since patients will increasingly deal with doctors trained to be political activists instead of true medical professionals.”
There is simply no evidence to support the claims that social factors are the cause of healthcare disparities. Michigan Med must explain why it is committed to spending money from the state’s taxpaying citizens on initiatives that clearly contribute nothing toward developing competent physicians, while perpetuating the DEI agenda.
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_2150211137-scaled.jpg13502560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-12-01 11:42:412026-02-11 15:33:41University of Michigan Medical School Invoices Show Taxpayer Dollars Spent on Lectures That Indoctrinate, Not Educate
An email exchange between the West Virginia University (WVU) Health Science Center director of diversity and associate dean for admissions reveals the officials are determined to pursue admissions practices that, they believe, will provide a higher rate of minority students and still allow them to work around Republican legislative control.
Documents obtained by Do No Harm through Freedom of Information Act (FOIA) requests show that, on July 17, 2023, WVU Associate Dean for Admissions and Student Affairs Mary Euler, PharmD, emailed Courtney Lanham, the school’s director of diversity with this question:
In our last Executive Committee meeting, one of our chairs was concerned about using “DEI” for our initiatives because of the Legislative tension. He feels it puts a target on us. It was suggested that perhaps we change our committee to the Inclusivity Committee with the same goals and actions. Has any other committee raised this concern?
The exchange continued:
Lanham: No they have not. I can pose this to VP Poore and see what she thinks. I do not have a strong opinion either way as long as the work gets done.
Euler: Me either and I am not afraid to have a target on my back for something I so strongly believe is necessary. Keep me posted.
Lanham: Diversity is much more than affirmative action though. So as long as we clearly define what we mean by it, I feel confident. We stripping affirmative action upthrows all of our practices, I have to wonder if we were doing it correctly to begin as well. This is an opportunity for us to restructure how we approach diversity.
Euler: I get it. Thanks.
Lanham: Thank you for being so amazing.
WVU’s Health Sciences website, which covers the schools of dentistry, medicine, nursing, pharmacy, and public health, currently promotes the diversity, equity, and inclusion (DEI) tenet of “health equity.”
“Our future providers must mirror our global population,” WVU says. “We recognize racism is a public health crisis and we’re empowering our campus to learn more and take action.”
“When we are more diverse, we are more creative and innovative,” the school claims, adding that diversity “creates a sense of belonging and appreciation” that is believed to translate to “a culture of inclusive excellence.”
Figure 1. From “WVU Libraries Office Anti-racism Collection in Overdrive” (June 29, 2020).
The FOIA documents also show Lanham forwarding to colleagues a letter from a nonprofit civil rights organization warning the school would be breaking the law if it fails to comply with the Supreme Court’s ruling that found race-based admissions practices unconstitutional.
Besides the potential legal issues surrounding the continuation of race-based admissions practices, medical schools that have embraced DEI ideology are already facing a decline in quality.
In a letter to the Wall Street Journal editorial board in February, Do No Harm Chairman Stanley Goldfarb, M.D. commented on the numerous schools of medicine that have made the choice of abandoning the U.S. News and World Report rankings due to their failure to maintain academic excellence as they joined others who jumped on the political DEI train.
To schools like WVU, that have adopted the radical doctrine that “our future providers must mirror our global population,” Goldfarb wrote:
There is no evidence that minority students who are qualified to enter medical school are being denied admission. While the Liaison Committee on Medical Education has required medical schools to increase the diversity of their classes for several years, the number of minority students has increased only minimally and remains well below the sought-after goal of equaling the proportion of blacks in America.
“Medical schools have had to confront the fact that an insufficient number of qualified students are available,” Goldfarb asserted. “Forcing greater diversity therefore must lead to a reduction in the merit of the students accepted.”
https://donoharmmedicine.org/wp-content/uploads/2023/09/shutterstock_124304896-scaled.jpg15362560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-30 13:17:322026-02-11 15:33:41West Virginia University Health Sciences Center Hides Its DEI Work to Avoid Legislative Oversight
The California State Board of Pharmacy says it “shall not renew a pharmacist license” unless the license holder has successfully completed a course in “cultural competency and humility” that focuses on Critical Race Theory-inspired ideology.
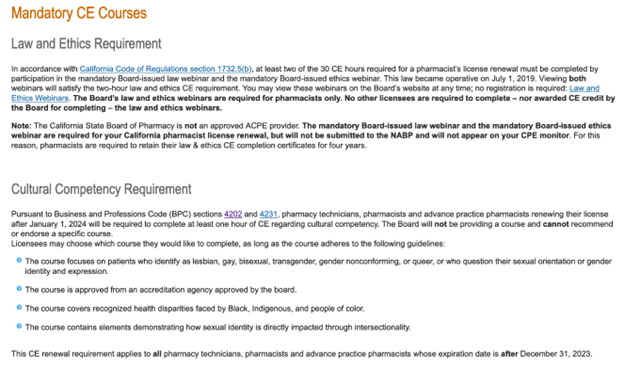
An anonymous tip obtained by Do No Harm shows the state board is now requiring pharmacists and pharmacy technicians to complete the diversity, equity, and inclusion (DEI) training. “Pursuant to Business and Professions Code (BPC) sections 4202 and 4231, pharmacy technicians, pharmacists and advance practice pharmacists renewing their license after January 1, 2024 will be required to complete at least one hour of CE regarding cultural competency,” the board statesunder its section on “Mandatory CE Courses.”
Figure 1. Mandatory continuing education requirements for California pharmacists.
“The Board will not be providing a course and cannot recommend or endorse a specific course,” the directive continues, but adds the board requires the DEI training “adheres to the following guidelines”:
The course focuses on patients who identify as lesbian, gay, bisexual, transgender, gender nonconforming, or queer, or who question their sexual orientation or gender identity and expression.
The course is approved from an accreditation agency approved by the board.
The course covers recognized health disparities faced by “Black, Indigenous, and people of color.“
The course contains elements demonstrating how sexual identity is directly impacted through intersectionality.
License holders must submit to the board “proof satisfactory” which “may include specifying completion of the required CE on the renewal application provided by the Board,” says the email sent by the anonymous source.
Figure 2. Email sent to California pharmacists regarding the mandatory continuing education (October 19, 2023).
In August, Pacific Legal Foundation filed a lawsuit on behalf of Dr. Azadeh Khatibi, Dr. Marilyn Singleton, and Do No Harm, that challenges California’s mandatory Critical Race Theory-inspired implicit bias training for physicians, asserting such mandates are unconstitutional. Now, these mandates are clearly being extended to other healthcare fields.
Khatibi v. Lawson, filed in the U.S. District Court for the Northern District of California, argues:
Rather than respect the freedom and judgment of continuing medical education instructors to choose which topics to teach, California law now requires the Medical Board of California to enforce the mandate that all continuing medical education courses include discussion of implicit bias. Under the First Amendment to the United States Constitution, the government cannot compel speakers to engage in discussions on subjects they prefer to remain silent about. Likewise, the government cannot condition a speaker’s ability to offer courses for credit on the requirement that she espouse the government’s favored view on a controversial topic. This case seeks to vindicate those important constitutional rights.
“Physicians should base medical care on each patient’s individual situation and condition,” Caleb Trotter, an attorney at Pacific Legal Foundation, said in a press statement about the case. “Implicit bias training does the opposite, telling doctors they should be concerned about a patient’s immutable characteristics like race, gender, and sexual orientation, regardless of the characteristics’ relevance to the patient’s treatment.”
Singleton, a California anesthesiologist who teaches continuing medical education courses in the state, and also serves as a visiting fellow at Do No Harm, said the mandatory implicit bias training “promotes the inaccurate belief that white individuals are naturally racist.”
“This message can be detrimental to medical professionals and their patients as it creates an atmosphere of suspicion and animosity, which goes against the fundamental principle of doing no harm,” she continued.
Do No Harm Chairman Dr. Stanley Goldfarb emphasized that physicians are not merely agents of the state.
“Physicians have free will and act in the best interest of their patients,” he said in the press statement.
“The idea of unconscious bias states that one acts on those biases, and there’s no evidence of this happening in the medical community,” Goldfarb added. “Medical professionals take the Hippocratic oath to do no harm, and do not need lawmakers or medical organizations to tell them what they should think when providing medical advice to patients.”
Goldfarb’s words readily apply across healthcare disciplines, including the field of pharmacy.
The August meeting minutes of the California State Board of Pharmacy show that, in July 2022, board staff attended training “on building an inclusive regulatory community.” In July 2023, the state board reported that 20 “executive level, senior management and management staff” completed a day-long DEI training that included:
Introduction to Cultural Intelligence
Understanding Implicit Bias Through the Lens of Cultural Intelligence
Managing Conflict Through the Lens of Equity
How to Create Sustainable Change
Also in July, the minutes indicate board staff completed additional training courses that included “How to Decode Our Unconscious Bias.”
Despite these clear references to DEI training in the board’s meeting minutes, there is no mention of mandatory DEI training for license renewal in the state pharmacy board’s “Strategic Plan” for 2022-2026.
https://donoharmmedicine.org/wp-content/uploads/2023/11/shutterstock_717437125-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2023-11-29 14:46:202026-02-11 15:33:41California State Board of Pharmacy Mandates ‘Cultural Competency’ DEI Training for License Renewal