
Dr. Stanley Goldfarb and Dr. Benita Cotton-Orr examine the two paths that our healthcare system can take as we move ahead to the future, including considerations for access and how improving access leads to better outcomes.
Dr. Stanley Goldfarb and Dr. Benita Cotton-Orr examine the two paths that our healthcare system can take as we move ahead to the future, including considerations for access and how improving access leads to better outcomes.

A recent and well-publicized article in the New England Journal of Medicine (NEJM) declares that juveniles begun on sex-characteristic altering hormones experience increased satisfaction with their physical appearance and improved psychosocial functioning. Yet this isn’t the full story. An accompanying editorial outlines the continued uncertainties about the potential adverse effects of these drugs on adolescents going through puberty. In fact, there are many uncertainties and weaknesses of this study that should be addressed.
The researchers and four clinics featured in this study have a well-publicized history of radical activism and advocacy for the medical transition of children. For example, Boston Children’s Hospital posted and later removed a video on its YouTube channel that endorsed the idea that some children know their gender identity “from the womb.” As we noted in our recently released study, the UCSF website endorses the idea that naturopathic providers are well-suited to prescribe gender-affirming hormones. Lurie Children’s Hospital of Chicago has disseminated “educational” materials to local schools that recommends that schools “automatically ‘affirm’ students who announce sexual transitions, and ‘communicate a non-binary understanding of gender’ to children in the classrooms…to disrupt the ‘entrenched [gender] norms in western society.'” One co-author of the paper based at Children’s Hospital Los Angeles told CNN in 2014 that “We’re definitely in the middle of a gender revolution and it’s exciting.”
Given this obvious bias, there is a high likelihood that study participants were steered toward responses that align with the activism promoted by these clinics. This phenomenon – known as “demand characteristics” – is a remarkably well-documented threat to the validity of survey-based scientific inquiry, even for researchers who do their best to conduct studies dispassionately and objectively.
The study suffers from other major flaws, as well. Its results indicate that the only meaningful improvement over time was participant scores for “appearance congruence.” Improvement in positive affect, life satisfaction, depression and anxiety only improved by the smallest margins. Notably, their study does not include comparison groups that received psychotherapy or no intervention, so whether these modest improvements are superior to alternative approaches is impossible to assess.
The researchers observe extremely modest self-reported mental health improvement among participants who began taking gender-affirming hormones later in puberty, but static measures among those who started taking these hormones early in puberty. They explain that “These observations align with other published reports that earlier access to gender affirming medical care is associated with more positive psychosocial functioning.” In other words, they assert that the lack of improvement among this subsample constitutes evidence in support of their radical worldview. It’s a “heads I win, tails you lose” proposition.
This study, despite the headlines it has received, is fatally flawed and borderline unscientific. Like other studies on the topic, it obfuscates rather than clarifies questions around the medical transition of children. Policymakers must accept that elite gatekeepers have become cheerleaders and that their recommendations on politicized topics warrant healthy skepticism. Rather than follow their lead, policymakers should emulate European countries that increasingly prohibit access to these experimental treatments for minors, largely due to acknowledgement that the evidence base fails to establish that these treatments are beneficial on balance.
American children deserve better than risky medical treatments justified by activism cloaked as research. Until reform comes, the “adults in the room” might just be on another continent.
The American Medical Association (AMA) promoted its January 28-29, 2023 “Physicians of the Future Summit” as an opportunity “to learn essential skills to become leaders in organized medicine.” So why did the summit help medical students “promot[e] equity”?
The opening speaker of the plenary session was Dr. Camara Phyllis Jones, who is “well-known for her allegories on race and racism.” Her presentation, Achieving Health Equity: Habits of Mind for Social Justice Warriors, promised to give medical students the skills and tools necessary “to navigate valuing and prioritizing social justice work.” Apparently, that’s essential for the physicians of the future.
She has written about this topic in other publications and has presented it in various venues. The “Dual Reality” allegory refers to the two-sided nature of the “open/closed” signs seen at restaurants everywhere. Dr. Jones claims that “racism creates two-sided signs in our society” and therefore, a dual reality. She states, “It is difficult for White people in the United States to recognize white privilege and racism.” How is this information helpful to medical students?
The AMA needs to return to its stated mission “to promote the art and science of medicine.” Leave the woke indoctrination out of professional development events for medical students – present and future alike.
Have you received promotional materials from professional healthcare associations that promote wokeism? Let us know via Do No Harm’s secure portal.
Just how woke is the State University of New York (SUNY) Downstate Health Sciences University College of Medicine (HSU COM)? The wokest of all, as it just confirmed to Do No Harm.
Here’s the background. In November 2022, the Association of American Medical Colleges released a report showing that the vast majority of medical schools have embraced identity politics, despite their divisive and even discriminatory nature. The report was based on surveys of specific medical schools, which the AAMC didn’t name.
For the sake of transparency and accountability, Do No Harm submitted freedom of information requests to public medical schools nationwide, including SUNY Downstate College of Medicine. We asked for a copy of its survey response, so that New York taxpayers and policymakers could learn the truth about this institution.
Here’s what the SUNY Downstate HSU COM has self-reported:
All told, the SUNY Downstate Health Sciences University College of Medicine has instituted 100% of the divisive and discriminatory woke policies listed by the AAMC – the first perfect score we have seen. And you can bet it will respond to pressure from activists and outside groups to go even further down the radical rabbit hole – doing even more damage to faculty, medical students, and ultimately, the millions of patients they’ll see.
New York taxpayers help fund the SUNY Downstate HSU COM. They, and the policymakers who represent them, should ask why they’re giving so much money to an institution that’s putting divisive and discriminatory ideology at the heart of medical education. More importantly, they should ensure the COM stops, and soon.

The Society for Evidence Based Gender Medicine (SEGM) recently announced the publication of a new study titled The Myth of Reliable Research in Pediatric Gender Medicine. This research examined two well-known Dutch studies that strongly influenced the practices that came to be known as “gender affirming care” for minors.
The Dutch studies contain “three methodological biases” that undermine the research, the authors said. First, only the “most successful cases” were included in the outcomes. Second, the finding of “resolution of gender dysphoria” was based on faulty measurement methods pre-/post-treatment. Finally, the authors noted that the simultaneous use of psychotherapy, hormone therapy, and surgery “made it impossible to separate the effects” of each intervention.
SEGM says that the new study “demands urgent attention from the medical community” due to the risk of harm to youth in the United States and worldwide, particularly in the Western world. “The authors highlight how far the field of gender-medicine has drifted from the core principles of evidence-based medicine,” the organization said in a statement published on its website. “The gender medicine field has a limited time to self-correct before public health authorities, and increasingly, elected officials who do not understand medicine but do understand the risks of harm to youth, step in to curb the damage.”
Because the circumstances are so critical, Do No Harm recently launched its Protecting Minors from Gender Ideology initiative. This effort serves to educate policymakers, healthcare professionals, and the public on the disastrous consequences of inflicting unproven interventions onto children in the name of “gender-affirming care.” We are fighting back against the narrative of misinformation and attempts to discredit the actual scientific evidence that gender ideologues engage in. Exposing the errors and defects of long-accepted “research” is an early step in protecting children from these dangerous practices.
SEGM is a non-profit organization and a group of more than 100 clinicians and researchers with a mission to raise the bar on the quality of evidence in gender medicine, with a focus on children, adolescents, and young adults.

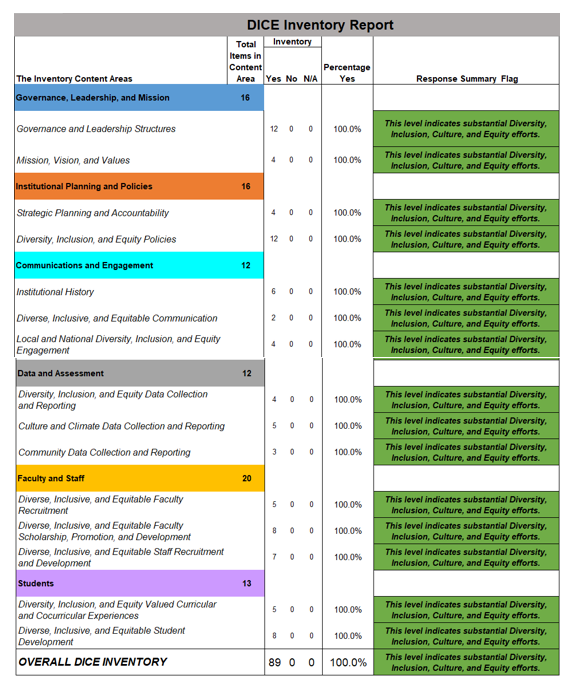
The Purdue College of Health and Human Sciences is home to several departments and schools dedicated to health professions, including the School of Nursing. And, as a tipster recently informed us, it is also home to a robust program that is dedicated to diversity, equity, and inclusion. In fact, DEI is “core to the mission and values” of the College of Health and Human Sciences.
Not to be outdone, the School of Nursing builds upon that mission by claiming, “Nursing stands at the intersectionality of healthcare and social justice” and that “systemic racism is still pervasive” in the profession.
To address these issues, the Purdue School of Nursing created a council for students, faculty/staff, and community members with the aims of “eliminating systemic racism and promoting DEI.” The school embeds this agenda into its curriculum, including an “emphasis” on DEI in courses that are traditionally among the fundamentals of undergraduate nursing education, such as:
This emphasis carries over into graduate nursing courses like Clinical Application of Pharmacotherapeutics and Acute Illness: Pediatric Health Preceptorship. Are the actions of medications in the human body now a legitimate target of the woke mob?
The need for appropriately trained nurses in the healthcare industry is well documented. Depending on residency status, the cost of attendance to Purdue University ranges from almost $10,000 to more than $28,000 per year. Students who are paying these tuition rates to enter a much-needed profession deserve to receive an education that actually prepares them to advocate for patients, not for woke ideologies.
Is your nursing school or academic program being invaded by wokeness? Do No Harm wants to hear from you via our secure platform.

Does Fluffy or Furball need a woke veterinarian? At Tennessee’s Lincoln Memorial University, the answer is apparently yes. A tipster recently sent us details about a faculty and staff workshop from its Richard A. Gillespie College of Veterinary Medicine. It shows that divisive and discriminatory ideology has infected this part of health care, too.
The workshop was entitled “Inclusivity,” and according to the accompanying press release, it was “designed to educate the veterinary community on diversity, equity, inclusion, [and] belonging.” What any of this has to do with caring for animals is left unstated, but then that’s the point. This is about indoctrination more than veterinary education.
Naturally, Lincoln Memorial University doesn’t stop there. It also has so-called “BLEND Diversity Training” as part of its “Master of Veterinary Clinical Care” program. It’s filled with typical woke assertions about the lack of diversity and the need to fixate on people’s skin, especially in recruitment:
“The veterinary profession is one of the least diverse professions in the country,” said Associate Professor and MVCC Director Bonnie Price. “The U.S. population is becoming more diverse, and Gen Z is the most diverse generation in history. Veterinary medicine must diversify and support our workforce, build our professional knowledge… and tailor veterinary health care to the cultural needs of all pet owners.”

It’s a safe bet that Tennessee’s Lincoln Memorial University’s veterinary school isn’t alone. Such is the nature of the woke takeover of health care. It won’t rest until it has complete control over every facet of medicine – even veterinarians who treat dogs and cats.
Have you seen woke ideology in your corner of health care, from acupuncture to physical therapy to anything in between? Please let us – securely and anonymously.

Three cheers for Utah: The Beehive State just protected children from radical transgender treatments. This common-sense policy is compassionate and evidence-based, and more states should take up this issue for the sake of vulnerable kids.
Utah’s new law, authored by Sen. Mike Kennedy and Rep. Katy Hall, overwhelmingly passed the state legislature last week. Gov. Spencer Cox signed it on Saturday. It prohibits all gender-reassignment surgeries for children and ends hormone therapies, as well. These treatments are known to be invasive and are often irreversible, while potentially causing serious health challenges, including strokes, heart attacks, and cancer. The law creates strong legal protections for children who are harmed by these treatments.
The new law also calls on the executive branch to conduct a systematic review of the evidence on hormone therapies on minors. If this review is conducted properly, it will undoubtedly conclude that the risks outweigh the benefits, and that children should be protected from these harmful procedures.
Sure enough, that’s what the most progressive European countries have already concluded, as Do No Harm has shown. Gox. Cox acknowledged this fact when signing the law: “More and more experts, states, and countries around the world are pausing these permanent and life-altering treatments for new patients until more and better research can help determine the long-term consequences.”
Thanks to this new law, Utah children who believe they are transgender are much more likely to receive the medical care they need, including psychotherapy sessions. That stands in stark contrast to typical American approach – pushed by radical activists – of treatments and surgeries as quickly and as early as possible. Research has shown that most children who believe they are transgender do not maintain that belief into adulthood, while existing mental health issues that contribute to this feeling deserve to be addressed in therapy.
Naturally, trans activists are savaging Utah and trying to stop other states from following its lead. But policymakers nationwide should ignore them and look to Utah for inspiration. Vulnerable children deserve better than radical gender ideology. They deserve compassion and caution, and Utah deserves praise for giving it to them.

A North Carolina doctor reached out to us with this story – a story that should both worry fellow physicians and inspire them to action. We are keeping the doctor’s identity anonymous for the sake of the individual’s protection.
One of the things I love about medicine is its collaborative nature. That’s why I applied for hospital privileges as an adjunct clinical faculty member at my local medical school. I wanted to help train the next generation of physicians, using my years of experience in medical practice to guide others in our life-saving work.
But it wasn’t to be. I ended up refusing the position – because I would have been forced to take radical woke training.
After I applied, I was quickly accepted and then directed to the orientation process. The very first training I was told I had to take was, you guessed it, about “diversity, equity, and inclusion.” I looked through the materials, and it was clear that a political agenda was being shoved down my throat. It was obsessed with race and skin color – not medical care and patient well-being.
That’s bad enough, but the fact that it was literally the first training is even worse, to my mind. My local medical school is sending a dangerous message to faculty: You’re here to be a political activist first, and a physician second. I can’t think of anything more inappropriate in the medical field. And that mindset will infect everything medical students learn and ultimately do as physicians. The quality of care will suffer if medical training focuses on anything other than treating patients.
I refuse to be a part of this. Within minutes of receiving the training, I decided to turn down hospital privileges. I emailed the Department Chair about my decision and gave my reasons. Weeks later, I have yet to hear a response.
Health care leaders may be silent and complicit, but I won’t be. And I hope my fellow physicians will speak out, too. The only way to stop the woke takeover of medicine is to stand up and say “not me.” If enough of us fight back, we have a chance to win the war for the heart of health care. Our patients are counting on us to stop this woke onslaught before it’s unstoppable.
Have you been forced to take woke training, or even refused to do so? Please let us know – securely and anonymously.

Why are so many elite medical schools leaving the famous US News and World Report rankings?
In recent weeks, the medical schools affiliated with Harvard, Pennsylvania, Stanford, Columbia, and many other prestigious institutions have taken this strange path. The reason is as simple as it is concerning: These schools are more committed to woke ideology than medical excellence.
These medical schools are more-or-less honest about what they’re doing. The Icahn School of Medicine at Mount Sinai said its commitment to “commitment to anti-racism” and “outreach to diverse communities” compel it to leave the rankings. The University of Pennsylvania Perelman School of Medicine said the rankings “measure the wrong things.”
Really? US News and World Report rankings are based in large part on MCAT scores and grade point averages of accepted medical school applicants. These measures are the best known indicator of students’ ability to excel in medical school, which is why US News started ranking them in the first place. The whole point is to help medical schools select and train the best possible future physicians.
Yet these institutions are less concerned with training the best physicians because of woke demands for diversity. Penn put it bluntly when announcing its decision. It stated: “The USNWR measures encourage the acceptance of students based upon the highest grades and test scores… The Perelman School of Medicine aims to serve the needs of a changing world, including diverse communities and stakeholders ranging from prospective students to the patients who rely on the physicians, scientists, and leaders we train.”
In other words, merit doesn’t matter. Academic achievement doesn’t matter. Subjective criteria apparently do. Yet that inevitably means that Penn will recruit students who don’t perform as well on academic and testing criteria. Eliminating the rankings allows them to take in less-qualified students.
Penn is not alone. Elite medical schools are now obsessed with skin color, and they want to recruit more lower-performing minority students without having their rankings hurt. Therefore, they left the rankings, so they can pretend to be elite while lowering standards.
This turn of events should worry every patient – which means every American. The nation’s top medical schools are deliberately downplaying merit in recruiting future physicians. Lowering standards is a surefire path to lower the quality of care that patients receive for decades to come. As Penn said, “The USNWR rankings perpetuate a vision for medical education and the future physician and scientist workforce that we do not share.” It should be deeply concerning that elite medical schools don’t share the vision of training the best possible medical professionals.
When Americans look at a medical school that isn’t participating in the US News and World Report rankings, they should think to themselves: This medical school is a threat to my health.

The Accreditation Council for Graduate Medical Education (ACGME) in a non-profit organization that “sets and monitors” educational standards in medical residency and fellowship programs. Accreditation is granted by ACGME’s Institutional Review Committee, which evaluates the data provided by the graduate medical education programs it oversees.
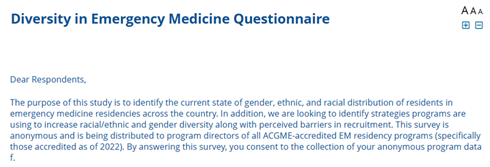
One method the ACGME uses for collecting those data points is by sending questionnaires to the program directors of various residencies in the United States. We obtained a copy of the “Diversity in Emergency Medicine Questionnaire,” which aims to “identify the current state of gender, ethnic, and racial distribution” of residency programs across the country. It also wants to know what program directors are doing to “increase racial/ethnic and gender diversity” in their recruitment efforts. Those who received a link to the questionnaire were assured that the study was approved by the Baylor College of Medicine Institutional Review Board, and 25 participants had the chance to receive a $100 Amazon gift card.
For assistance with their responses, program directors were instructed to refer to their “ERAS data.” ERAS® is the Electronic Residency Application Service® from the Association for American Medical Colleges (AAMC) and is said to “support the transition to residency in a fair and equitable way.”
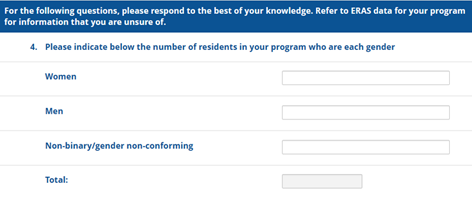
After determining which region of the country the program is in, the survey asked for “the number of residents in your program who are each gender.” A choice of “non-binary/gender non-conforming” is included.
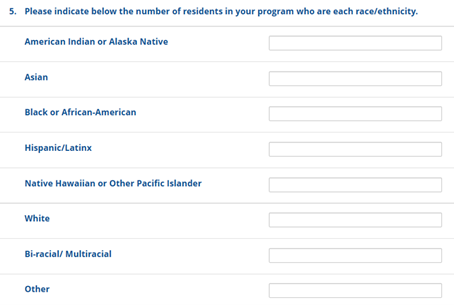
The next question inquires about the number of residents by race/ethnicity, including “American Indian or Alaska Native; Asian; Black or African-American; Hispanic/Latinx; Native Hawaiian or Other Pacific Islander; White; Bi-racial/Multiracial; Other.”
The ACGME seeks to further slice and dice the data by requesting the gender and race/ethnicity totals for the program’s chief residents.
In a series of required responses, the rest of the Diversity in Emergency Medicine Questionnaire focused on recruitment and initiatives to increase diversity. Program directors were asked to rank the importance of several elements of the “process of screening/interview selection of applicants” to the residency program, such as grades, test scores, “Underrepresented in Medicine (URiM) Status,” and “gender/gender identity.” Choices of strategies to promote DEI initiatives included:
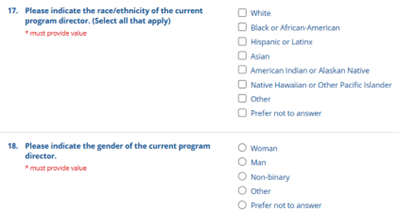
To complete and submit the questionnaire, the program manager was asked to provide an answer for his or her race/ethnicity and gender.
Why is the ACGME so obsessed with conducting research on the demographic data of the residency programs it accredits? The Program Director Guide to the Common Program Requirements provides some context:
It is expected that programs, in partnership with their Sponsoring Institutions, have and implement policies and procedures related to recruitment and retention of individuals underrepresented in medicine and medical leadership in accordance with the Sponsoring Institution’s mission and aims. The population of individuals considered underrepresented in medicine will include racial and ethnic minority individuals reflective of the program’s service area but may also include others the program deems underrepresented in medicine in the service area or in the discipline in general.
Further, the Guide directs readers to the ACGME Equity Matters™ initiative for “continuous learning and process improvement” in DEI and anti-racism. The resources in this program include “commitments to equity for making meaningful change,” and are intended to demonstrate “historical and current injustices in the medical education system.”

Clearly, the ACGME seeks to impress upon its residency program directors that advancing DEI and anti-racism over merit is of greater importance than providing the best emergency medicine training experience to new doctors.
Are you seeing a greater emphasis on DEI than medical learning in your residency program? Let us know – anonymously and securely.

Medical school deans are supposed to focus on teaching students to be the best physicians. The Indiana University School of Medicine has a different vision. IUSM just named its first “first executive associate dean for diversity, equity, inclusion and justice,” who will also serve as “Chief Diversity Officer.” The whole point of this job is to embed woke ideology even deeper at IUSM.
The new dean is Chemen M. Neal, who has already spent significant time promoting divisive ideas since her hiring in 2011. Yet now she’ll take this work to an unprecedented level. IUSM has announced that she will “lead an existing team of faculty and staff and have direct responsibility for a variety of areas, including”:
Note the complete lack of focus on medical education. There’s also significant overlap among these tasks, which points to the bureaucratic nature of the work. IUSM is growing a massive bureaucracy that will likely influence everything the medical school does.
What’s more, Neal has made clear that her goals include “establishing metrics to help school leadership gain a greater understanding of key areas like retention and belonging, as well as a focus on the diversification of faculty.” Translation: She wants to hire faculty based on skin color, instead of medical and teaching expertise. Medical students – and the patients they will treat – deserve better.
IUSM is already one of the most woke medical schools in America. We’ve documented how faculty must prove their woke credentials in order to get tenure or promoted. Now, with this new executive associate dean, IUSM is doubling down on the politicized transformation of medical education. Indiana policymakers may want to look into what IUSM is doing – and ask its leadership why such corruption of mission is justified.

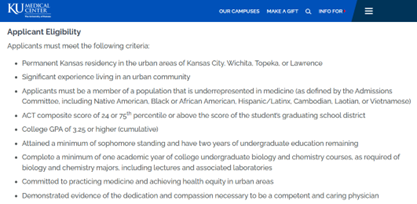
In August 2022, we reported that the University of Kansas School of Medicine and KU Medical Center offered a racially discriminatory program through its Office of Diversity and Inclusion. The eligibility criteria for the Urban Scholars Program for Students Underrepresented in Medicine state, “Applicants must be a member of a population that is underrepresented in medicine (as defined by the Admissions Committee, including Native American, Black or African American, Hispanic/Latinx, Cambodian, Laotian, or Vietnamese).” Placing race-based restrictions on a publicly funded program is a clear violation of Title VI of the Civil Rights Act, which prohibits such discrimination.
The school announced the Urban Scholars program in a press release that reiterated the eligibility restrictions and “guaranteed admission to KU School of Medicine” for students who successfully complete it.
In response to the complaint filed by Mark Perry, senior fellow at Do No Harm, the U.S. Department of Education’s Office for Civil Rights has opened an investigation into this discriminatory program. “The University of Kansas Medical School’s illegal race-based discrimination is representative of the widespread discrimination taking place at almost every US medical school on the basis of race, color, and/or national origin,” Perry said. “By emphasizing racial diversity over merit and academic ability for admission to the racially discriminatory Urban Scholars Program for Students Underrepresented in Medicine, KU School of Medicine is compromising its fundamental academic responsibilities to pursue instead an ideologically driven diversity agenda.”
Have you been excluded from a scholarship or fellowship program due to discriminatory eligibility criteria? Do No Harm wants to hear from you.

Do No Harm has announced its latest initiative “Protecting Minors from Gender Ideology,” an effort to educate policymakers and the public on the disastrous consequences of the unproven and often harmful practice known as “gender-affirming care.”
“Gender-affirming care” is based on the premise that children and adolescents know best whether their feelings of discomfort with their bodies should be grounds for “treatment” with risky and experimental drugs and surgeries.
Do No Harm is committed to ensuring children who are diagnosed with, or believe they have, “gender dysphoria” are treated with the utmost care, caution, and concern.
“The movement to promote ‘gender affirming care’ is profoundly dangerous and driven by ideology rather than evidence,” said Dr. Stanley Goldfarb, MD, chairman of Do No Harm. “At their core, medical professionals who support these efforts are violating the Hippocratic oath directive to ‘do no harm’ by ignoring key consequences of this type of ‘care,’ including the fact that underlying mental health concerns are usually not addressed.”
Dr. Goldfarb notes that so-called “gender-affirming care” ignores the impossibility of informed consent for the child: “The procedures themselves can lead to physical impairment, including a lack of bone strength and brain maturation, and the loss of fertility. ‘Gender transitioning’ prior to maturation can lead to sexual dysfunction, including atrophy and necrosis of genital tissue, chronic pain, incontinence, and the inability to orgasm.”
As part of this launch, Do No Harm is releasing a new white paper, drafted with the help of Cooper & Kirk, PLLC, explaining the harms of these life-changing medical procedures and a comprehensive report identifying the different legal requirements for sex change-related treatments and actions between the US and western European countries.
In addition, Do No Harm is providing model legislation, “The JUST FACTs Act” (The JUSTice for Adolescent and Child Transitioners Act) to legislators in multiple states who want help navigating this challenging issue. The model legislation:
Finally, Do No Harm has engaged a number of well-respected senior fellows, including physicians, parents, patients, and detransitioner Chloe Cole, to share their medical expertise and personal experiences dealing with gender ideology through testimony and public presentations.
About Do No Harm
Do No Harm is a diverse group of physicians, healthcare professionals, medical students, patients, and policymakers united by an ethical mission: Protect healthcare from a radical, divisive, and discriminatory ideology. They believe in making healthcare better for all – not undermining it in pursuit of a political agenda. Learn more at www.donoharmmedicine.org

Just how woke is Tennessee’s UT College of Medicine? Very woke indeed, as it just confirmed to Do No Harm.
Here’s the background. In November 2022, the Association of American Medical Colleges released a report showing that the vast majority of medical schools have embraced identity politics, despite their divisive and even discriminatory nature. The report was based on surveys of specific medical schools, which the AAMC didn’t name.
For the sake of transparency and accountability, Do No Harm submitted freedom of information requests to public medical schools nationwide, including the UT College of Medicine (UTCOM). We asked for a copy of its survey response, so that Tennessee taxpayers and policymakers could learn the truth about this institution.
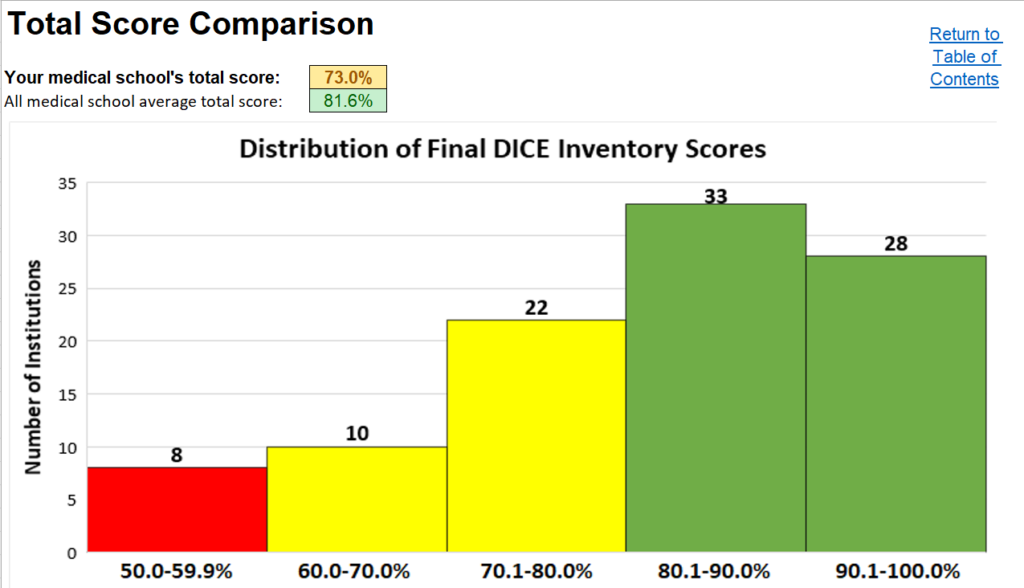
Here’s what the UT College of Medicine has self-reported:
All told, the UT College of Medicine has instituted 73% of the divisive and discriminatory woke policies listed by the AAMC. This indicates that “moderate DEI efforts have been made.” And you can bet it is feeling pressure from activists and outside groups to go even further down the radical rabbit hole – doing even more damage to faculty, medical students, and ultimately, the millions of patients they’ll see.
Tennessee taxpayers help fund the UT College of Medicine. They, and the policymakers who represent them, should ask why they’re giving so much money to an institution that’s putting divisive and discriminatory ideology at the heart of medical education. More importantly, they should ensure the University of Tennessee College of Medicine stops, and soon.

We received a tip from a physician who works for Novant Health in North Carolina. The physician wanted to highlight a concerning development at their hospital and asked to remain anonymous. Here is the story.
My hospital wants patients to know how woke I am. It’s a blatant attempt to coerce me to broadcast political views. My fellow physicians and I are not only insulted but deeply worried about our careers because of this blatant coercion.
Here’s the backstory. I recently got an email from my hospital’s parent organization asking if we would like for our online profile to include a ‘LGBTQ friendly’ stamp. The stamp is rainbow colored and flashes under the doctor profiles.
In one respect, the stamp is meaningless. It was offered as a “grandfathered-in” certification, with or without any training or actual certification. Yet in a bigger sense, it’s filled with meaning. If I don’t adopt this stamp, my hospital gives patients the impression that I’m bigoted and hateful. It may even be grounds to push me and my colleagues out of the medical profession.
This move is concerning on so many levels. First of all, who in the medical practice is NOT LGBTQ friendly? Are there actually doctors who are unfriendly to their patients because of their sexual orientation? Of course not.
I’m a case in point. LGBTQ patients score me very high on patient satisfaction. Every physician and nurse I work with provides the highest level of care to these patients. This is our job and we don’t need a politicized stamp to prove anything. Yet if we don’t take it, we will somehow be ‘assumed’ to be unfriendly to LGBTQ people.
Something much more sinister could be at work. I fear an attempt to label people who will later be weeded out. Frankly, I’m terrified for my job if I don’t take the stamp. And I know dozens of my fellow physicians feel the same way. Medicine is heading in a dark direction, with physicians more worried about who they’ll offend than how to provide the best possible care.
Such are the wages of woke medicine: More posturing and politics, less professionalism and personalized care. I can’t imagine anything worse.
Is your hospital or health care provider forcing you to adopt woke views? Please let us know – securely and anonymously.

The U.S. Department of Education’s Office for Civil Rights (OCR) has opened an investigation into illegal race-based discrimination at the University of Missouri School of Medicine (MUSOM).

OCR is investigating Mizzou for ten university-funded scholarships in the School of Medicine that contain race/ethnicity restrictions for applicants, which is prohibited under Title VI of the Civil Rights Act of 1964:
The investigation was initiated in response to a federal civil rights complaint filed in August 2022 by Do No Harm program manager Laura Morgan.
MUSOM’s financial aid office says, “Most scholarships received by medical students are institutionally funded from donations and gifts from alumni and friends of our school.” Donors to the School of Medicine must insist their gifts are used for scholarships that are fair, open to all, and compliant with federal law.

We at Do No Harm are devoted to combating divisive ideology in health care. To date, we’ve focused on the rise of race-based medicine, most notably Critical Race Theory and the diversity-industrial complex that endanger patients by lowering standards and demanding discrimination. Now, another destructive ideology demands our attention – so-called “gender affirming care.” The health and happiness of countless children are at stake, which is why we’re now fighting to curtail this unscientific and individually harmful practice.
Race-based medicine and “gender-affirming care” arise from the same distorted view. In both cases, patients are viewed as part of a group, instead of unique individuals with unique medical challenges, including psychological ones. In the case of race-based based medicine, minority patients are seen as victims of oppression, which leads to disparate health outcomes, instead of individuals with specific health issues and treatment needs. As for “gender-affirming care,” it holds that any child who questions his or her sex should automatically be given the benefit of the doubt, instead of first identifying and treating underlying or contributing medical problems. In both cases, medical associations are quick to demand adherence to this view, while dismissing any counter-arguments – a clear sign of elevating political ideology over individual patients.
The refusal to approach each patient on an individual basis is reason enough to oppose the movement toward “gender-affirming care.” Yet there’s another reason it deserves criticism: It ignores the impossibility for informed consent of the children who are subjected to this approach. Put simply, young children and adolescents are inappropriately being allowed to make potentially irreversible life-altering decisions.
“Gender-affirming car involves several treatment stages. First, children as young as 6 to 8 years are encouraged to change their names, their hair styles, and their dress to enable their belief that they are the opposite sex. Then, as early as 8 to 10 years, they are treated with drugs called puberty blockers to prevent the development of secondary sex characteristics that develop during puberty. As early as 13 to 15 years, they begin hormonal treatments that lead to secondary sex characteristics of their desired gender. Finally, and once again as early as 13 to 15 years old, they can receive surgical procedures like mastectomies, genital revisions, and plastic surgery.
These procedures are not cost-free. To the contrary: They can lead to altered bone development and cognitive maturation, and even infertility and the inability to engage in sexual relations. It is dangerous and destructive to let children, whose minds are still developing, make decisions at such young ages.
Then there’s the lack of scientific research – a key component to sound medical treatment. No one knows the risk/benefit ratio for these procedures. No one knows how many children decide to reaffirm their biological sex in the middle of these procedures, during which time their minds are developing and maturing. And no one knows how many of these patients ultimately regret their decisions and are left with devastating alterations in their psyches and bodies.
What we do know is this: As few as 12% of children who believe they are a different gender continue to hold that view as adults. Yet the gender-affirming care model assumes that 100% will maintain this belief, while subjecting them to invasive and often irreversible medical procedures. While these children may feel supported and even satisfied for a few months after entering even the earliest stages of the treatment, the longer-term results are unknown and unstudied, and the likelihood is that they’ll wish they had waited before pursuing such a drastic course. Overall, the lack of evidence makes informed consent on the part of children impossible to obtain.
To be clear, adults who decide to undergo “gender transition” have the right to pursue such treatments. But children do not. In holding this position, Do No Harm parallels the best medical judgments of most European countries, including Sweden, Finland, and the United Kingdom, which have abandoned the “gender-affirming care” model precisely because it endangers children. European countries have largely adopted a first step of intense psychological assessment and counseling, which makes sense. If there is an underlying condition or medical need, it should be addressed first, instead of jumping straight to life-altering treatments.
Sadly, the United States refuses to take this common-sense approach. At best, psychological assessments are a quick pro-forma step with no chance of derailing a gender transition. In fact, the American Academy of Pediatrics and transgender activists oppose any delay in providing gender-affirming care, including the cautious and thoughtful assessment of depression, eating disorders, and other underlying problems that have been found in many children seeking synthetic transition. As a result, compared to Europe, the U.S. offers treatments like puberty blockers and sex-reassignment surgeries to patients at a much younger age and with much less mental development. The U.S. is an outlier – and children are being victimized because our country puts ideology ahead of individual patients.
Do No Harm is committed to ensuring that children who believe they have Gender Identity Disorder are treated with the utmost care, caution, and concern. We are working closely with experts in Pediatrics, Psychiatry, Endocrinology and Social Sciences to assess the literature on this topic and identify the path forward, both for medical practice and government policy. Yet this much is already clear: The U.S. should follow Europe’s lead and abandon “gender-affirming care” for children, instead applying a more individualized and medically accurate approach. In the same way that Do No Harm fights for equal access to care, and against divisive race-based medicine, we will fight to protect children from the dangerous ideology of “gender-affirming care.“