The Alliance for Continuing Education in the Health Professions (ACEHP) is an organization for healthcare educators, offering support and resources for their professional development offerings and activities, including continuing medical education (CME). However, ACEHP is doing its part to drag the delivery of healthcare continuing education into the endless abyss of DEI and anti-racism.
As it demonstrated during its recent annual conference (sponsored in part by CME providers such as Talem Health, Healio, and CME Institute), ACEHP’s idea of best practices includes a “DEI Showcase” of woke topics.

Examples of the February 7, 2023, sessions include:
- Are We Committed to DEI Progress or Are We Committed to DEI Notoriety? Dr. Russell Ledet urged attendees to learn how medical conditions appear “in people of color as opposed to white people,” and discussed how DEI progress appears versus “what is just for clout.” To “make DEI progress from a CME perspective,” Dr. Ledet recommended Harriet Washington’s book on Medical Apartheid (which says that experiments within certain black populations is “a tradition that continues today”) and The 1619 Project (which claims America’s founding was not in 1776, but based on the year slaves arrived in Virginia) as helpful resources.
- Infusing Diversity, Equity, Inclusion, and Anti-racism [DEIA] Concepts Into the Fabric of Continuing Education. As the institution that “is leading the important conversations on DEIA,” the University of North Texas Health Science Center at Fort Worth presented a “learning lab” for incorporating DEIA concepts into the planning, delivery, and evaluation phases of continuing medical education. The session aimed to “foster the critical thinking and self-awareness of the participants” with case studies that encourage the application of DEIA principles into mission statements, planning committees, and CME program operations.
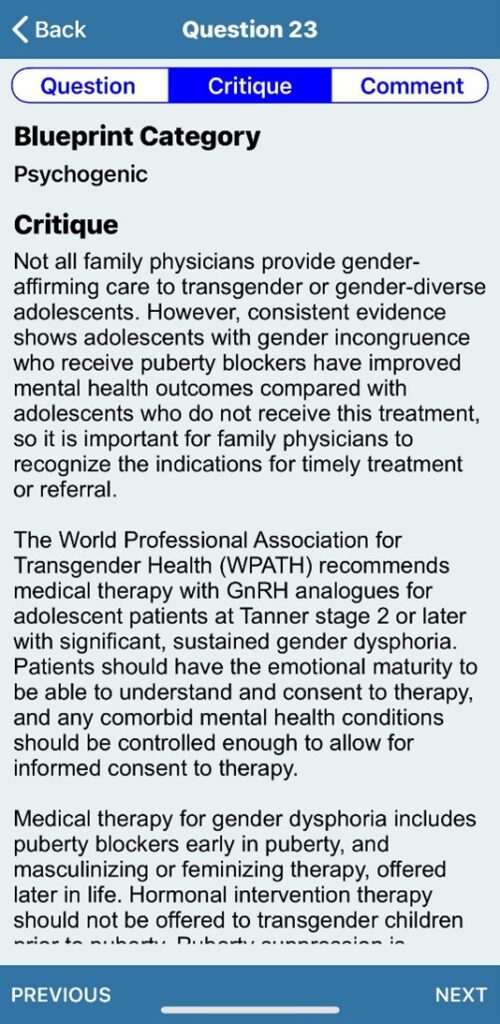
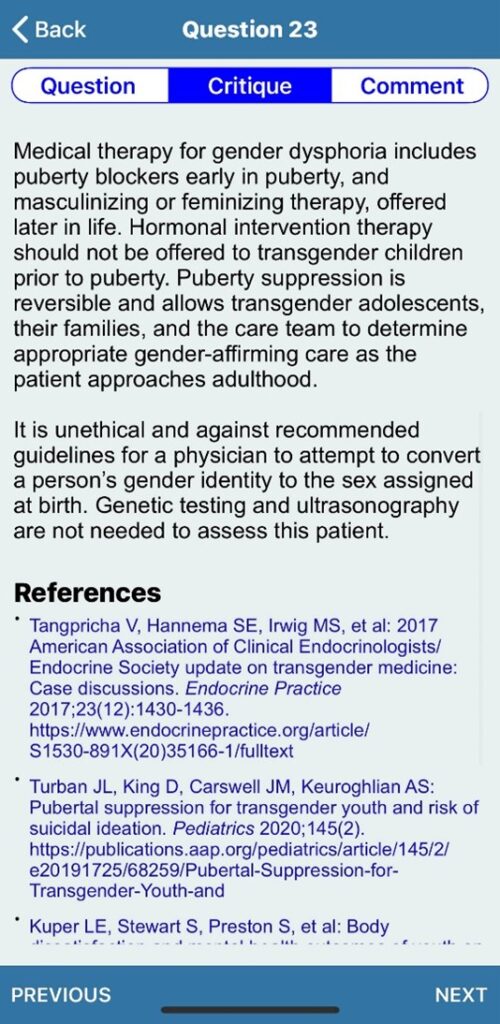
- Panel Discussion on Education that Improves Inclusive Healthcare: Lessons From a Program Focused on Cancer Screening and Care for Transgender Individuals. The presentation included “examples of DEI education that changes “healthcare professional] behavior.” In addition to a Q&A with the panel, this session presented clips from the documentary “Trans Dudes With Lady Cancer.”
- Learning Collaborative – Driving Equity Through Awareness: Addressing Social Determinants of Health and Disparities in Care in Medical Education. Panelists advised attendees on methods to incorporate health equity information into their continuing education offerings, and how to discuss “challenging” topics with patients so they “feel more comfortable and trust their healthcare professionals.”
Policy & Medicine, a website that reviews and writes about healthcare-related regulatory and compliance issues, endorsed the conference, particularly the day dedicated to health equity. While praising the objectives of the sessions, their coverage included a curious reflection. “We must know more than that there is an issue and develop a plan,” the author said, “to ensure everyone is treated with dignity and respect and deliver the care patients deserve.”
Yet this is not the message of DEI activists, who push an ideology that declares the healthcare industry is systemically racist and certain groups of practitioners must be trained to recognize and mitigate their implicit biases. ACEHP and its members need to apply the standards of dignity, respect, and competent patient care delivery to the field of continuing professional development instead of redefining the meaning of best practices and creating discord in the healthcare industry.
Is your professional healthcare organization promoting divisive ideologies instead of adhering to the mission of providing competent patient care? Do No Harm wants to hear from you, and you may remain anonymous if you wish.