The Alliance for Academic Internal Medicine(AAIM) states that it “promotes the advancement and professional development of its members,” who are involved in educating future internal medicine (IM) physicians.
Considering that IM specialists are experts in diagnosis and non-surgical treatment of patients with complex medical conditions, it’s vital for the most qualified candidates to enter this field.
Yet, AAIM appears to be more interested in achieving “equity” over merit in undergraduate medical education (UME). The August 2025 edition of AAIM’s “Diversity Now” newsletter references an October 14 webinar on “Enhancing Equity in Assessment within the UME Grading Process – A Data Driven Approach.”
This document outlines desired changes for the assessment of IM clerkship participants so that “no one is disadvantaged from achieving [their full learning] potential because of structural or social barriers.”
Faculty must complete training in “implicit bias” and “microaggressions” on an ongoing basis to “mitigate against potential effects of the individual bias of those responsible for assigning grades.”
But that isn’t enough to achieve equity, according to the AAIM:
If standardized exams are used in clerkship grading, limit the weight that standardized exam scores, including National Board of Medical Examiner’s subject or shelf exams, have in determining a student’s grade. Differences between population group outcomes in standardized examinations likely reflect unequal opportunities afforded to underrepresented in medicine (UIM) students. In addition, deemphasizing exam scores might allow students to shift their attention to other important patient skills that they need to develop.
This is a remarkable statement. Essentially, AAIM is arguing that merit and achievement should be devalued, because focusing on these objective metrics of competency might disadvantage certain racial groups.
This naturally compromises the quality of medicine to advance perverse ideological goals, and drives everyone – of all races – to mediocrity.
And, although the original work for these recommendations was published in 2021, AAIM continues to host the materialon its website.
AAIM’s proposed grading reforms represent more than procedural adjustments. They signal a willingness to subordinate merit-based assessment to identity-based considerations in the name of equity.
The question is straightforward: Should medical students be evaluated primarily on their clinical competency and medical knowledge, or should assessment systems incorporate identity-based considerations to achieve predetermined demographic outcomes? The answer has profound implications for the future of IM education and, ultimately, the quality of patient care.
https://donoharmmedicine.org/wp-content/uploads/2024/12/shutterstock_2491577653-scaled.jpg17092560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-16 22:05:362026-02-11 15:34:17How AAIM’s Equity-Based Grading Reforms Threaten Merit and Competency in Medical Education
Recently, the Centers for Medicare & Medicaid Services (CMS) incorporated proposals by Do No Harm and Defending Education in a final ruleestablishing additional protections to keep unlawful discrimination out of medical residency programs for graduate medical education.
These protections are aimed at preventing graduate medical education accreditors, like the Accreditation Council for Graduate Medical Education (ACGME) and others, from requiring or otherwise encouraging or promoting hospitals to implement discriminatory criteria in their medical residency programs.
Under the final rule, hospitals may continue to receive federal payments for direct and indirect graduate medical education costs for accredited medical residency programs.
However, for payment purposes, CMS will only deem an accredited program “approved” where the accreditation organization “does not use accreditation criteria that promote or encourage discrimination on the basis of race, color, national origin, sex, age, disability, or religion, including the use of those characteristics or intentional proxies for those characteristics as a selection criterion for employment, program participation, resource allocation, or similar activities, opportunities, or benefits.”
In practice, this means that accreditors continuing to force discriminatory standards in accreditation requirements for graduate medical education will place accredited hospital programs at risk by imposing potentially significant financial burdens to hospitals, who may not be able to recoup costly graduate medical education expenses.
The final rule’s implementation of these anti-discrimination provisions directly reflects the language Do No Harm and Defending Education proposed in acomment to the agency earlier this fall.
In September, Do No Harm submitted a responsive commentto CMS’sproposed rule, warning the agency that the rule’s anti-discrimination protections may be susceptible to circumvention in which accreditors “engag[e] in word play to circumvent the proposed rule’s reach.”
Given various, ongoing circumvention efforts, our comment laid out the very real possibility that accreditors might easily evade the rule through word gaming and cosmetic changes that merely cloak the continued practice of DEI.
As Do No Harm has documented in our “Zombie DEI” report and elsewhere, many institutions simply rebrand their DEI programs and initiatives while continuing to engage in racially discriminatory practices and promote radical identity politics.
CMS took our concerns seriously.
Indeed, in issuing the final rule, CMS explicitly credited these concerns as motivating its decision to revise the final language.
The agency further stated that it “agree[s] that the regulations should more explicitly specify the types of practices that will be prohibited under [the] finalized policy,” confirming that CMS would “add language to the regulations that would prevent accreditors from engaging in word play as a means of circumventing the proposed policy.”
Do No Harm applauds CMS for taking action to address this urgent problem in medical education.
The role of accreditors in injecting racially discriminatory policies and practices not just in graduate medical education, but throughout medical and healthcare education, is often overlooked. But accreditors, due to the immense power they wield, can effectively extort these programs into implementing DEI policies as a condition of accreditation.
Do No Harm’s March report on medical and healthcare education accreditors highlighted this dynamic.
We examined ten such accreditors, including the Liaison Committee on Medical Education (LCME), the Council on Podiatric Medical Education (CPME), and the Commission on Dental Accreditation (CODA), and found that each of them imposed various DEI mandates upon professional healthcare degree programs.
These ranged from explicit requirements to maintain DEI offices and programs to more indirect encouragement of efforts to achieve certain diversity-related outcomes.
And in April, the Trump administration took notice of this problem; President Trump issued an executive order directly targeting discriminatory accreditation standards in medical education.
The order specifically directed the Department of Justice, the Department of Education, and the Department of Health and Human Services to “investigate and take appropriate action to terminate unlawful discrimination by American medical schools or graduate medical education entities that is advanced by the Liaison Committee on Medical Education or the Accreditation Council for Graduate Medical Education or other accreditors of graduate medical education, including unlawful ‘diversity, equity, and inclusion’ requirements under the guise of accreditation standards.”
Following the executive order, many of the accreditors began to ditchovert language in their accreditation standards that required medical and healthcare education programs to implement DEI policies and/or engage in racial discrimination.
For instance, in May, the LCME voted to eliminate Element 3.3, a requirement that forced medical schools to have in place “programs and/or partnerships” aimed at achieving diversity.
And in September, the ACGME not only eliminatedDEI requirements from its accreditation standards, but closed its DEI department.
CPME, another accreditor of graduate medical education,suspendeddiversity requirements for podiatric medical colleges and residency programsfollowing the executive order.
The CMS final rule implements crucial protections to cleanse graduate medical education of unlawful DEI mandates, including shutting down surreptitious discrimination in accreditation standards advanced by entities like the ACGME and CPME. Such a rule is necessary given these institutions’ long histories of DEI activism.
The ACGME has been particularly vocal in its endorsements of DEI: back in 2024, the ACGME’s then-DEI officer bemoanedefforts to disband DEI programs as “insane.”
And at its 2023annual education conference, the ACGME hosted no fewer than 11 sessions dedicated to advancing DEI in medical education.
These examples underscore the need for strong federal action to ensure that DEI is removed from medical and healthcare education.
In summary, the CMS rule is a crucial step forward toward ridding graduate medical education of harmful racial discrimination.
https://donoharmmedicine.org/wp-content/uploads/2023/08/shutterstock_1919186000-scaled.jpg17092560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-15 21:04:202026-02-11 15:34:17CMS Takes a Crucial Step Toward Ridding Medical Education of DEI
Last year, the University of Maryland School of Medicine (UMSOM) unveiledits new strategic plan for 2025-2030.
But unfortunately, the plan is replete with commitments to promote identity politics in medical education.
Goal 4 of the school’s “Community” sub-plan is for the school to “[l]ead the city, state, and national conversation on mitigating health disparities and improving health equity.”
Perhaps in a vacuum, to a person unfamiliar with the “equity” jargon employed in medicine and medical education, this goal might not seem so troubling. But as Do No Harm has demonstrated, “health equity” is often interchangeable with efforts that seek to equalize outcomes between racial groups through discrimination.
Indeed, when the plan provides more granular detail on how UMSOM will achieve this goal, it’s clear that these efforts will encompass ideological indoctrination.
For instance, the school aims to “[i]ntegrate concepts of health equity, anti-racism, population health, community care, and social determinants of health into curricula”; additionally, it will “[d]eliver training modules on antiracism, health equity, and social determinants of health to educate any UMB faculty, student, or staff member involved in a community project.”
To highlight just a few issues with these goals, “anti-racism” as understood by its most prolific proponent, Ibram X. Kendi, essentially seeksto address systemic racism in society through racial discrimination.
Social determinants of health, meanwhile, refer to the pseudoscientific concept that differences in social and economic conditions cause disparities in health outcomes between certain groups. Although there is certainly a correlation between these conditions and health outcomes, the “social determinants of health” theory is at best oversimplified and ignores other factors such as individual agency and health decisions that contribute to health outcomes.
If these goals seem like mere distractions that don’t reflect UMSOM’s core institutional commitments, think again.
Elsewhere in the strategic plan, UMSOM pledges to “[c]ommit resources to become a national leader in health equity research” and to “[e]xamine all current and emergent generational health challenges through the lens of health equity.”
UMSOM is about as clear as it can be that identity politics is the primary means by which it understands its role in medical education.
Additionally, UMSOM aims to engage in what can only be described as quasi-political activism.
For instance, the strategic plan includes pledges to “[e]ngage with community leaders, Baltimore City Fire Department, and the UMB Community Engagement Office to identify community priorities and barriers to care”; “[c]reate documentaries, educational videos, and media toolboxes in partnership with Baltimore’s emergent Black film makers to highlight the needs and successes, as well as to amplify the voices of the West Baltimore community”; and “[f]oster and grow a cohort of students, faculty, and staff committed to restorative justice and motivated to ensure health equity.”
It intends to recruit students in these efforts as well; one pledge is to “[i]nvolve students in purposeful community outreach, clinical care, and partnered programs.”
Ethical considerations aside, this is simply not the role of a medical school; UMSOM’s goal should be to train the best physicians possible, not delve into local politics.
In summary, this strategic plan reveals a profound, institutional infatuation with identity politics and a willingness to inject these ideas into students’ learning experiences.
UMSOM should ditch these goals at once and affirm its commitment to providing the best medical education possible.
https://donoharmmedicine.org/wp-content/uploads/2023/01/shutterstock_549470497-scaled.jpg14402560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-15 20:29:382026-02-11 15:34:17University of Maryland’s Med School Has a Strategic Plan: Go All In on ‘Health Equity’ and Anti-Racism.
For years, Do No Harm has sounded the alarmover the false and misleading claims promoted by the child transgender industry and echoed by major medical associations.
Too often, these organizations refuse to meaningfully engage with studyafter study finding a lack of credible evidence to support sex-denying medical interventions for minors.
And too often, these organizations gloss over the harms and consequences of life-altering medical procedures, insteadfalsely downplaying their severity.
Now, it seems like for some organizations, their history of promoting dangerous and misleading statements may be catching up with them.
Earlier this week, Florida Attorney General James Uthmeier announced a lawsuitagainst the World Professional Association for Transgender Health (WPATH), the Endocrine Society, and the American Academy of Pediatrics, accusing them of violating Florida law prohibiting unfair and deceptive trade practices.
The lawsuit points to the organizations’ promotion of sex-denying medical interventions for children, which lack credible evidence to support their use.
In 2023, @GovRonDeSantis signed legislation to ban so-called "gender-affirming care" for kids. Now it’s time for accountability!
— Attorney General James Uthmeier (@AGJamesUthmeier) December 9, 2025
The lawsuit highlighted the claim that puberty blockers are “reversible” as an example of a deceptive statement.
Puberty blockers can cause diminished bone density in minors, with research showingthat they negatively affect “bone mineral density, especially at the lumbar spine, which is only partially restored after sex steroid administration.” Artificially preventing a child from going into puberty is inherently experimental.
Moreover, research shows that nearly all children subjected to puberty blockers go on to take cross-sex hormones, which carry long-term risksof infertility and impaired sexual function.
“The years-long coordinated campaign by WPATH and other medical organizations to disregard the serious health risks of sex change interventions on minors will go down as the most egregious medical scandal in modern history,” said Do No Harm Medical Director Kurt Miceli, MD.
“These groups have obfuscated risk and misrepresented the low quality of evidence to support puberty blockers, cross sex hormones, and surgeries for children—interventions that can cause lasting harm,” said Dr. Miceli. “It is encouraging to see our elected officials hold these organizations accountable for spreading misinformation.”
Accountability is a critical step to restoring public trust in medicine.
https://donoharmmedicine.org/wp-content/uploads/2024/08/shutterstock_2387894327-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-11 21:34:092026-02-11 15:34:17Is Accountability Finally Coming for the Child Transgender Industry?
RICHMOND, VA; December 11, 2025 –Today, Texas Attorney General Ken Paxton announced a lawsuit against electronic healh record company Epic for allegedly engaging in deceptive practices that restrict parental access to their children’s medical records.
The lawsuit follows a report from Do No Harm earlier this year explaining how hospitals and electronic health record companies have worked to undermine parents’ access to their children’s medical information. According to the Texas Attorney General’s announcement, Epic automatically hides certain information about a child’s medical history from parents when the child turns twelve years old.
Do No Harm Medical Director Kurt Miceli, MD, issued the the following statement in response:
“A recent reportby Do No Harmrevealed how woke electronic health record vendors like Epic are limiting parents’ ‘proxy’ access to their children’s medical records. It is encouraging to see Attorney General Ken Paxton hold Epic accountable for placing children directly in harm’s way by removing parental protections, allowing activist physicians to funnel minors into the gender cult without parental knowledge or consent. This lawsuit is a critical step to restoring lawful parental access to their children’s medical records during their child’s developmental years.”
Do No Harm’s full report on parental access to their children’s medical records is available here.
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. It has over 50,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 14 countries.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-11 19:30:102026-02-11 15:34:17Do No Harm Medical Director Issues Statement in Response to Texas Health Record Lawsuit
The Perry Initiative, an organization that previously promoted women-only talent development programs in the field of orthopedics, has now opened its programs to all.
The Perry Outreach Program offers students the chance to engage with “hands-on mock orthopaedic surgeries, biomechanical engineering experiments, and interactive talks from prominent engineers and surgeons.” The Medical Student Outreach Program provides students with the opportunity to “hear from residents and attending surgeons, discuss pathways into orthopaedic surgery, and participate in hands-on surgical skills sessions.”
However, the programs previously required applicants to identify as “female or non-binary” to be eligible for the program. Indeed, the initiative’s motto previously was: “Building the Pipeline for Women in Engineering and Medicine.”
This is, of course, blatant and illegal discrimination on the basis of sex.
So, back in 2023, Do No Harm submitted a federal civil rights complaint against 12 medical schools that partnered with The Perry Initiative to advertise, promote, and/or host the programming.
Do No Harm’s complaint, filed with the Department of Education’s Office for Civil Rights, pointed out that universities promoting these programs were violating Title IX of the Education Amendments of 1972, which forbids federally-funded institutions of higher education from engaging in sex-based discrimination.
The schools named in the complaint are as follows:
Oklahoma School of Science and Mathematics
Yale University
Wake Forest University
New York University
University of New Mexico
University of Pittsburgh
Duke University
Albert Einstein College of Medicine
University of Arizona
University of Iowa
Oregon Health and Science University
University of Virginia
Later the same year, Do No Harm also filed complaints against the University of Minnesota, Indiana University, and the University of Delaware after similar programs were announced on their campuses. The Education Department’s Office for Civil Rights responded by opening federal investigations into many of the schools we flagged.
Now, following our complaints and the ensuing federal investigations, it appears The Perry Initiative has rethought its commitment to sex-based discrimination.
The information pages for The Perry Initiative programs make clear that these programs are now open to all, whereas before, it was clear that the programs were restricted to women.
Moreover, the Perry Initiative’s mission now states that it aims to build “the talent pipeline in the fields of orthopaedic surgery and engineering.”
All told, it’s an encouraging sign that The Perry Initiative is opening its programs to all. Following the efforts of Do No Harm, The Perry Initiative and its academic partners appear to have a better understanding that Title IX isn’t optional, and compliance isn’t voluntary: it’s legally mandated.
Sex-based discrimination has no place in healthcare training and education, and the field is best served when medical programs are open to all students and selection is based on merit.
https://donoharmmedicine.org/wp-content/uploads/2024/02/shutterstock_417195604-scaled.jpg17092560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-11 15:43:502026-02-11 15:34:17The Perry Initiative Ditches Discriminatory Criteria in Its Medical Programming Following Federal Civil Rights Complaints by Do No Harm
RICHMOND, VA; December 10, 2025 – This week, Jay Greene joins Do No Harm as the new Director of Research after serving as a senior fellow with Do No Harm for several years. In his new role, Jay will continue to support the fight against DEI and gender ideology as he oversees research projects that expose political agendas and harmful ideologies in the medical field.
Jay brings to Do No Harm an accomplished record of academic research that has had significant influence over public policy. Jay previously founded, led, and served as Distinguished Professor and Chair of the Department of Education Reform at the University of Arkansas. He has edited or authored five books and more than 40 peer-reviewed articles on a wide-range of topics.
“It is a privilege to take on this role with Do No Harm and work alongside its members as they fight against the harmful embrace of DEI in medicine and gender-affirming care interventions on minors,” said Greene. “Since first joining Do No Harm as a senior fellow, I have watched the organization lead the fight to restore merit and scientific rigor to the practice of medicine to regain the public and patients’ trust in medical schools, institutions, professional societies, and providers. I look forward to working alongside Ian Kingsbury and the entire Do No Harm team as we conduct thoughtful and credible research to reverse the corruption of the American medical field by political agendas.”
Much of Jay’s work over the years involved the pressing issue of antisemitism within medical institutions, and how DEI practices are often linked to antisemitic sentiments. Jay has also worked in concert with many of Do No Harm’s initiatives,co-authoring reports that debunk the racial concordance theory, contributing to podcasts calling out antisemitism in medicine, andrevealingthe deep bias and unreliable research conducted by major medical institutions.
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. It has over 50,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 14 countries.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-10 19:53:482026-02-11 15:34:17Do No Harm Welcomes Jay Greene as New Director of Research
DEI and wokeness in healthcare are a danger to medicine and lives. There’s no clearer case of this than the woke doctors who removed racial differences in kidney function, a move that messed up transplant lists and bumped critically ill patients down the waitlist behind less sick patients. Such wokeness is integrated into medical schools across the country, including UCLA, Wake Forest, and others. At UCLA, the woke standards mean students don’t know how to test for serious conditions like sepsis.
Now we can report that the same woke ideology is alive and well at the Indiana University School of Medicine (IUSM). In documents obtained by Do No Harm and shared with Townhall, it’s clear the school is teaching identity politics and pseudoscience instead of actual medicine.
https://donoharmmedicine.org/wp-content/uploads/2022/04/DNH_MediaHitGold_TownHall.jpg6301100Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-09 21:24:392026-02-11 15:34:17The Indiana University Medical School Hasn’t Ditched Wokeness Yet
Utah lawmakers will soon decide whether to keep laws in place protecting kids from transgender procedures. Their decision will be based in a large part on a report the Utah legislature commissioned — a report one watchdog says is “terribly flawed.”
Do No Harm on Tuesday released a memo highlighting the problems with a report commissioned by the Utah legislature on transgender procedures on kids. The memo, first shared with The Daily Wire, says that the report significantly misrepresents the scientific record and glosses over the danger of transgender procedures.
This month, Do No Harm Chairman Stanley Goldfarb, MD, joined the latest episode of the DonorsTrust Giving Ventures podcast to discuss the threats posed by identity politics to medicine and medical education.
Dr. Goldfarb explained how medical schools have de-emphasized traditional metrics of aptitude and achievement, such as grades and MCAT scores, in favor of DEI-related traits such as race and ideology. Increasingly, schools have shifted their focus toward advancing political agendas over educating the best possible physicians — to the detriment of patients everywhere.
Additionally, Dr. Goldfarb discussed the rise of the child transgender industry, diving into how, through a heavily-politicized process, medical providers are proposing dangerous medical interventions that lack credible evidence.
The discussion also covered Do No Harm’s various efforts, including policy work and litigation, to protect children and get identity politics out of medicine.
You can listen to thefull episodehere, and watch the discussion on YouTube as well.
https://donoharmmedicine.org/wp-content/uploads/stanpodcast.jpg5621139Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-09 18:59:552026-02-11 15:34:17Dr. Stanley Goldfarb Discusses Dangers of Identity Politics on ‘Giving Ventures’ Podcast
Do No Harm lays out five key areas where the Utah Report falls short:
The Utah Report fails to meet the basic requirements for being considered a systematic review.
While the report references a large volume of data, it fails to acknowledge the data’s low quality.
The Utah Report accepts so-called guidelines for so-called “gender-affirming care” from major medical organizations at face value without scrutinizing them, even though previous systematic reviews had debunked these “guidelines.”
The report neglects significant adverse side effects associated with “gender-affirming hormone therapy,” such as infertility, sterility, and sexual dysfunction.
The Utah Report required the Utah Department of Health and Human Services (UDHSS) to consult with “advisors” who promoted so-called “gender-affirming care” and failed to disclose their biases.
“This Utah Report is unreliable, unscientific, and fails to meet the standards of a systematic review,” said Michelle Havrilla, CRNP, Director of Programs – Gender Ideology for Do No Harm. “The Report’s inaccuracies and bias diminish its credibility and allow left-wing activists to weaponize it for their political machinations. Utah legislators must not rely on a report that clearly undermines the safety and well-being of minors.”
The UDHHS conducted the Utah Report in response to S.B. 16 Transgender Medical Treatments and Procedures Amendments, signed into law in January of 2023. Although the Utah Report spans more than 1,000 pages of academic and technical language, it relies on sheer volume rather than on the quality of the evidence.
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. It has over 50,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 14 countries.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-09 14:35:592026-02-11 15:34:17Do No Harm Report Debunks Utah Study on So-Called ‘Gender-Affirming Care’
Earlier this year, Duke University Health System and Duke University School of Medicine were under the magnifying glass for a host of discriminatory DEI programs and policies.
First, in March, Do No Harm submitted a federal civil rights complaint against Duke Health for racially discriminatory practices in its admissions and scholarship decisions. Duke Health’s diversity plan had explicitly called for adapting admissions processes to increase acceptance of underrepresented minority applicants, even pairing prospective minority candidates with current minority students during the admissions process.
What’s more, the Washington Free Beacon reportedin July that the School of Medicine had adopted promotion guidelines designed to “foster a diverse pipeline of potential learners from BIPOC and other marginalized groups” and “measurably increase the number of BIPOC learners.”
Next, Secretary of Health and Human Services Robert F. Kennedy, Jr. and Secretary of Education Linda McMahon demandedDuke Health end its discriminatory practices and implement measures to ensure merit is prioritized.
However, throughout 2025, Duke has undertaken something of a public-facing rebrand regarding DEI, scrubbing or moderating much of its more overt endorsements of race-based programming and identity politics.
For instance, Duke ditched its “anti-racism pledge” that featured attestations including a recognition of “our own implicit biases,” an affirmation “that excellent research and health care cannot happen without equity,” and a promise to “actively engag[e] members of diverse populations to guide and lead our research.”
And according to The Duke Chronicle, the School of MedicineshutteredDEI programs, including its “Inclusion, Diversity, Equity, Advancement and Leadership in the Sciences” or IDEALS office, in September.
The medical school also maintains the Office for Culture, Engagement, and Impact, which appears to be distinct from the Culture, Engagement, and Community program, despite similarities in name.
However, much objectionable programming remains within the Office for Culture, Engagement, and Impact.
The school’s “ME² Black Employee Resource Group,” for example, aims “to foster a community focused on networking, professional development, and leadership opportunities for Black staff.” Its webpage does include a disclaimer stating that all are welcome to attend its meetings, but a group focused on the professional development of a specific racial group is disturbing nonetheless.
Additionally, the school maintains an awards programthat recognizes contributions to “equity” and “inclusion.”
Given Duke’s long history of overt racial discrimination and the fact that much racialized programming remains, it’s hard to believe that these changes aren’t closer to cosmetic attempts at damage control rather than substantive, institutional shifts in the school’s priorities.
Duke should make clear, publicly and proudly, that it will no longer engage in any radical identity politics, and end its DEI programming for good.
https://donoharmmedicine.org/wp-content/uploads/dukemed.jpg5811144Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-09 13:39:552026-02-11 15:34:17Duke’s DEI Rebrand Leaves Something to be Desired
In December 2024, Do No Harm submitted an application to the Oregon Health Authority — the agency overseeing most of Oregon’s heath care programs — to provide a “cultural competency” training course. Basically, Do No Harm sought to provide a healthcare education opportunity that breaks down identity politics and replaces it with a focus on patients’ unique situations and clinical presentations.
As you can imagine, Oregon officials were not thrilled.
Perhaps the questions on their application form were a giveaway as to their attitude on DEI in medicine. For example, one question asked:
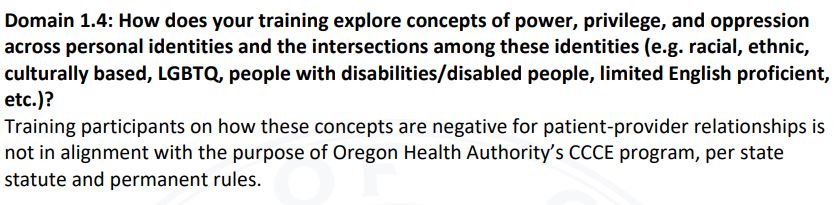
“How does your training explore concepts of power, privilege and oppression across personal identities? Please be inclusive of individuals who hold multiple social/cultural identities which intersect in unique ways for each individual (e.g. racial, ethnic, culturally-based, LGBTQ, people with disabilities, limited English proficient, etc.)?”
Translation: tell us what we want to hear, not what you actually believe. And, as expected, our responses were not what Oregon bureaucrats had in mind.
In their six-page rejection letter of Do No Harm’s application, the Oregon Health Authority described in great detail why Do No Harm’s course was not acceptable. In doing so, the Authority revealed its own bias.
Figure 1. An excerpt from the Oregon Health Authority’s rejection letter.
For example, the Authority noted “While evaluators appreciate the importance of focusing on the patient in the room and their specific needs, it seems harmful to not acknowledge implicit bias, systemic racism, and other forms of oppression, which very much impact a patient’s experience of the world and of the healthcare system.” They went on to assert that “The DO NO HARM organization appears to believe their counter perspective to be factual and any other perspective that does not align with their thinking as ‘ideological’ and without merit.”
In other words, DEI, implicit bias training, and racial concordance theories are “sound, scientific criteria.” But daring to question them is indicative of a “pervasive ideology.”
Maybe it’s the Oregon Health Authority who is being ideological, and not the other way around?
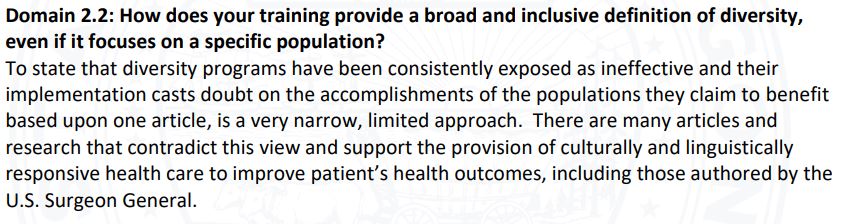
Figure 2. An excerpt from the Oregon Health Authority’s rejection letter.
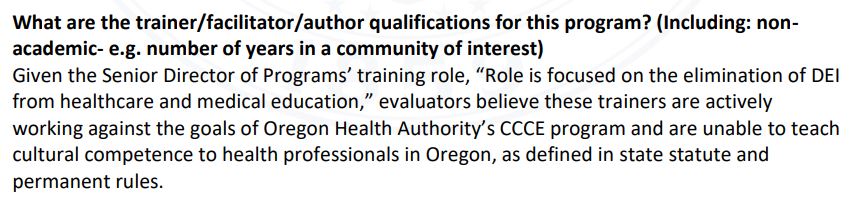
The rejection letter concluded by noting that “Given the Senior Director of Programs’ training role, ‘Role is focused on the elimination of DEI from healthcare and medical education,’ evaluators believe these trainers are actively working against the goals of Oregon Health Authority’s CCCE [cultural competence continuing education] program.”
Figure 3. An excerpt from the Oregon Health Authority’s rejection letter.
If the “goals” of the program are to indoctrinate healthcare professionals with DEI, treat woke concepts as indisputable facts, and dismiss any alternative viewpoint as a “pervasive ideology,” then perhaps the Authority has a point: Do No Harm does indeed dispute those goals.
None of this is entirely surprising given Oregon’s past missteps when it comes to medical regulation and licensure.
For example, in July 2024, Do No Harm reportedthat the Oregon Medical Board was seeking to revoke providers’ medical licenses if they were alleged to have engaged in “microaggressions.” Even doctors who simply failed to report microaggressions would have been stripped of licensure.
Just a few weeks later, the Oregon Medical Authority did a complete 180 and updated its proposed rule, with all references to “microaggressions” removed.
But while that reversal was encouraging at the time, the rejection of Do No Harm’s course application demonstrates that meaningful change among Oregon’s healthcare bureaucracy simply has not occurred. Rather than realizing that the concepts they are promoting are actively harmful — or even just permitting alternative viewpoints to be considered — officials have doubled-down on the same activist-infused standards that unfortunately are all-too-common among state healthcare agencies.
The sooner Oregon makes a real, substantive attempt to reverse course in a truly lasting way, the better. But until then, the underlying problems in Oregon’s healthcare environment will only grow worse.
https://donoharmmedicine.org/wp-content/uploads/2024/07/shutterstock_249441406-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-08 14:11:502026-02-11 15:34:17Do No Harm Applied to Provide Training in Oregon. State Officials Weren’t Pleased
The article by Lawrence, et al. echoes a recurring narrative in academic medicine: America’s history, dating back to colonial times, has created disparities that shape current racial health inequities, & in this case, cardiovascular (CV) health. The authors report that neighborhoods ranked highest on the Structural Racism Effect Index (SREI) have greater prevalence of hypertension, obesity, diabetes, smoking, & lack of physical activity.
Indeed, Lawrence, et al. single out structural racism as the explanation for these observed health disparities. By doing so they disregard other factors like geography, access, comorbidities, choice, & genetics. And while they acknowledge their study is limited by ecological fallacy, recall bias, & potentially missing covariates, they nevertheless conclude that CV risk factors and CV disease are associated with racism.
Dr. Stanley Goldfarb’s Doing Great Harm? isn’t another anti-woke broadside. It’s something rarer: a first-hand dispatch from a man who spent half a century inside the medical establishment, watched it lose its bearings, and decided to do something about it.
The story begins with his own cancellation at the University of Pennsylvania’s medical school and the online medical encyclopedia UpToDate, banished for the crime of asking whether lowering standards in the name of diversity might, in fact, harm patients. The fallout was predictable — what followed was not. Rather than retreat quietly, Goldfarb founded Do No Harm, a national network of physicians, nurses, and patients determined to push back against what he calls the “ideological capture” of medicine.
https://donoharmmedicine.org/wp-content/uploads/2022/07/DNH_MediaHit_WashingtonExaminer.png6311101Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-05 13:41:552026-02-11 15:34:16The fight to keep politics out of medicine
Earlier this year, Do No Harm published a report examining how parental access to their children’s medical records has been undermined by hospitals. The report also identifies the ways in which health records technology has been used to shield children’s health information from their parents.
For instance, major electronic health record system provider Oracle Health sets age 13 as the default protected status age, enabling providers to hide important health information from children’s parents.
As Do No Harm’s report notes, these restrictions pose enormous problems, as they could conceal harmful medical interventions such as so-called “gender-affirming care” from parents. Indeed, many gender activists who practice in the “Adolescent Medicine” subspecialty even advocate for limiting parental access to children’s medical records.
And what’s more, these restrictions are not in line with the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule that governs access to personal health information.
Now, the Department of Health and Human Services (HHS) Office for Civil Rights issued a Dear Colleague letterthis week reminding hospitals and other HIPAA-related entities of their obligations under the rule.
And according to the Daily Wire, HHS “was first made aware of ‘Adolescent Medicine’ and its dangers through a report issued by ‘Do No Harm.’”
“[P]arents, as the personal representative of their minor children, may be denied access to their minor children’s medical records, or a covered entity may be requiring minor children to authorize parental access before such access will be granted, when no such requirement exists under applicable law and, thus, under the Privacy Rule,” the letter states. “Denial of access in those circumstances may be a violation of the Privacy Rule.”
The letter reiterates the three limited situations in which a child’s parent is not eligible to access their personal health information:
When the child consents to health care and the consent of the parent is not required under state or other applicable law. In this situation, the parent is not the child’s personal representative with respect to PHI related to that health care.
When the child obtains health care at the direction of a court, or a person appointed by the court. In this situation, the parent is not the child’s personal representative with respect to PHI related to that health care.
When, and to the extent that, the parent agrees that the child and the health care provider may have a confidential relationship. In this situation, the scope of the parent’s agreement to the confidential relationship determines the degree to which the parent is the child’s personal representative for purposes of PHI maintained by that health care provider.
The letter goes on to state that, absent these exceptions and other conditions imposed by state law, hospitals may not prevent parents from accessing their child’s medical records.
“Providing parents who are their children’s personal representatives with easy access to their children’s PHI empowers parents to be more in control of decisions regarding their children’s health and well-being,” the letter states.
Do No Harm applauds HHS’s attention to this important issue. It’s essential that parents be able to access such crucial health information about their child. Preventing them from doing so infringes upon their core parental rights.
https://donoharmmedicine.org/wp-content/uploads/2022/06/shutterstock_797358901-scaled.jpg17042560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-04 22:52:482026-02-11 15:34:16HHS Reminds Hospitals: Let Parents Access Their Children’s Medical Records
HHS Office of Civil Rights Director Paula Stannard told The Daily Wire in a phone interview that the department was first made aware of “Adolescent Medicine” and its dangers through a report issued by “Do No Harm,” a group that fights back against gender ideology, and has raised many concerns about the medical community transitioning children without parental consent. Stannard called this activist push for “Adolescent Medicine” very “concerning,” particularly from her perspective and her role in enforcing HIPAA.
[…]
The HHS Office of Civil Rights is reminding health care providers, in very plain terms, of a parent’s right to access their child’s health information under the Health Insurance Portability and Accountability Act of 1996 (HIPAA) Privacy Rule, which states that a parent is the personal representative of their child and has the legal authority to make health care decisions for the child. In the department’s “Dear Colleague” letter, HHS emphasized that parents are indeed their children’s personal representatives and absolutely have the right of access to their child’s health information.
https://donoharmmedicine.org/wp-content/uploads/2022/04/DNH_MediaHit_DailyWire.png6311101Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-04 22:00:452026-02-11 15:34:16HHS To Investigate Midwestern School Accused Of Vaccinating Child Against Parents’ Wishes
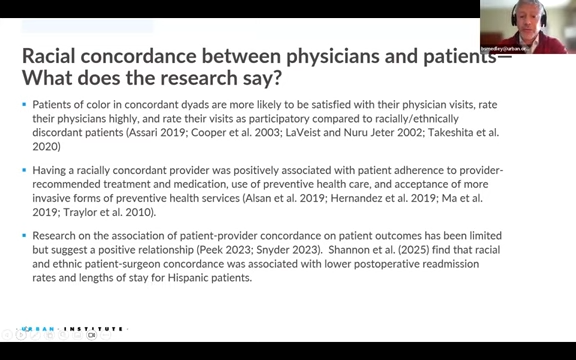
During a March discussionhosted by the Urban Institute and Georgetown University Law School, faculty members from law and medical schools discussed plans to continue “increasing physician diversity” through DEI initiatives.
The event, titled “Equal Protection and the Future of the Physician Workforce,” was premised on the notion that a decline in minority enrollment in medical schools, following the Supreme Court’s decision in Students for Fair Admissions v. Harvard (SFFA), would lead to negative health outcomes.
“[R]esearch shows that diversity among health professionals improves patient access, trust, and outcomes,” the event description reads. “Join the Urban Institute and Georgetown Law for a discussion of declining diversity in medicine, the worrisome health implications, and legal strategies for increasing physician diversity.”
To support this premise, Urban Institute Senior Fellow Brian Smedley overviewed a report, “Racially Minoritized Patients Can Benefit from Racially Concordant Providers but Struggle to Find Them,” which argued that racial concordance improves health outcomes and thus diversity initiatives in medicine are justified.
Figure 1. Screenshot of “Equal Protection and the Future of the Physician Workforce.”
The notion that racial concordance – when patients are treated by physicians of the same race – improves health outcomes is not supported by the preponderance of existing evidence; five out six systematic reviews find that racial concordance has no impact on health outcomes.
Moreover, the Urban Institute report cites along-debunkedstudy to justify its claims that racial concordance improves health outcomes. That study, “Physician–patient racial concordance and disparities in birthing mortality for newborns,” failed to control for the effect of very low birth weight on mortality; researchers at the Manhattan Institute attempted to replicate the study using the same data while applying that control, andfoundthat the racial concordance effect disappeared.
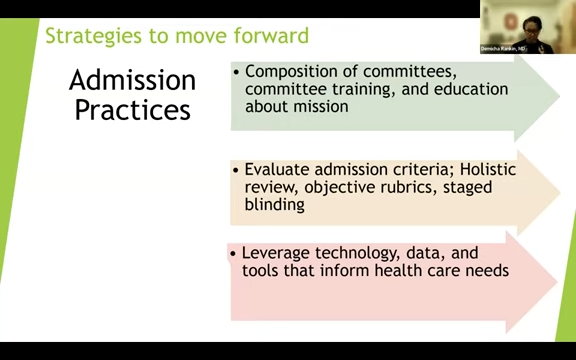
Next, Demicha Rankin, MD, the associate dean for Admissions at The Ohio State University College of Medicine, discussed ways in which medical schools could continue to diversify their student body, despite no longer being able to engage in racial discrimination in admissions.
These included recruitment and admissions strategies.
When discussing recruiting, Dr. Rankin argued that while the SFFA decision prevented racial discrimination in admissions, it did not prevent the targeting of race in recruiting outreach.
“In many instances, recruitment can be targeted for specific demographics, so long as it is open to all,” Dr. Rankin said.
Next, when discussing admissions decisions, Dr. Rankin appeared to argue that a more “diverse” admissions committee would lead to more diversity among accepted students.
“Really lean into who is on the committee, how can you diversify the committee, because if there’s representation there and if there’s broad-lived experiences, this can influence the decisions that a committee is making in terms of who is accepted,” she said.
Next, Dr. Rankin discussed how “holistic review” (in which admission is determined by weighing factors unrelated to academic achievement) could be a tool for diversifying the student body.
Figure 2. Screenshot of “Equal Protection and the Future of the Physician Workforce.”
“I think the biggest takeaway is leaning into holistic review,” she said. “It takes more than just a perfect MCAT or GPA to matriculate into medical school.”
“They also have to have compassion, empathy, resiliency, grit; and that is not measured by an academic metric,” she continued.
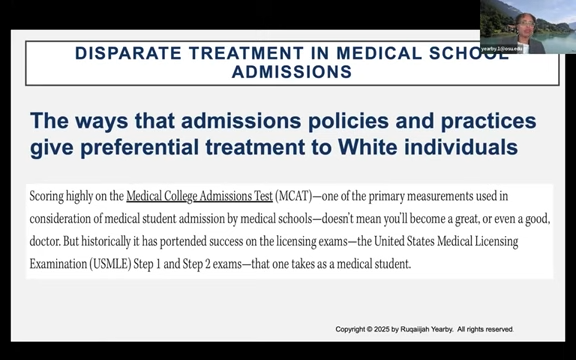
The next speaker, Ruqaiijah Yearby, a law professor at Saint Louis University, argued that medical schools should not “pre-comply” with guidance from the Trump administration to end discriminatory DEI practices, stating that schools that do so are “violating” federal and state antidiscrimination laws.
To be clear, racial discrimination in scholarships, funding decisions, and so on is illegal under the United States Constitution as well as federal civil rights law.
Next, Yearby argued that medical schools already employ “admissions policies and practices that give preferential treatment to white individuals, even though they are not connected to the ability of people to actually be great doctors.”
In explaining this point, Yearby pointed to the MCAT, with the apparent but unspoken implication that because white applicants tend to score higher on the MCAT than applicants of other racial groups, considering the MCAT gives preferential treatment to white applicants.
Figure 3. Screenshot of “Equal Protection and the Future of the Physician Workforce.”
This notion is truly disturbing. It does not logically follow that considering a test in the admissions process is somehow giving the group that performed better on that test a leg up.
Yearby’s argument would essentially treat any consideration of objective measures of merit as giving “preferential treatment” to whichever racial group happened to perform better. Any disparity would be evidence of bias. This is not sound reasoning.
Next, Yearby appeared to devalue the MCAT entirely, arguing that “research has shown that [high MCAT scores] does not necessarily track” to applicants with high MCAT scores “being great doctors.” She then argued to deprioritize the MCAT in admissions decisions.
It’s certainly true that one is not necessarily guaranteed to be a great doctor solely because of his or her MCAT score. Yet that is irrelevant; the question is whether MCAT scores correlate with the future ability to show clinical mastery.
“There is a strong correlation between MCAT scores and clerkship or ‘shelf’ exams, as well as United States Medical Licensing Examination (USMLE) clinical knowledge exams. This means that, in general, the better a student’s MCAT scores, the better they will perform in medical school and the more mastery of clinical knowledge they will exhibit. In short, students with better MCAT scores tend to be better medical students.”
Taken together, the comments of the event’s participants reveal a shocking and disturbing vision of medical education as a tool not for producing the best possible physicians, but for advancing the DEI agenda.
These ideas have no place anywhere near medical education.
https://donoharmmedicine.org/wp-content/uploads/2023/02/image-1.png3791484Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-12-04 18:33:522026-02-11 15:34:16Med School Official, Academics Plot Ways to Continue DEI Initiatives in Wake of Supreme Court Decision