Should medical school be reserved for the best and brightest or those who check arbitrary diversity checkmarks?
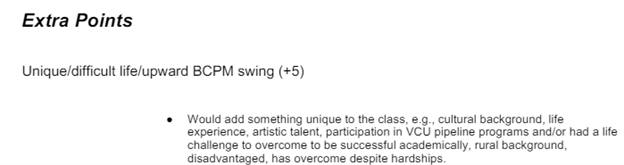
Last summer, the Supreme Court went a long way in clarifying the answer in ruling that race-conscious college admissions violate the Equal Protection Clause of the Fourteenth Amendment. The explicit racial favoritism that occurred in medical schools through affirmative action is (or at least ought to be) relegated to the dustbin of history. Unfortunately, the Court’s decision doesn’t mean that competence, excellence, and merit win outright. Admissions guidelines obtained by Do No Harm from the Virginia Commonwealth University (VCU) School of Medicine reveal that the school continues to reward “diversity.” Specifically, applicants receive additional points if they “would add something unique to the class (e.g., cultural background, life experience, artistic talent).”
Figure 1. From “File Review Guidelines for the 2023 Admissions Cycle,” page 5 (Virginia Commonwealth University).
The VCU guidelines offer no justification as to why the school values things like cultural background, rural habitation, or artistic talent, none of which predict clinical success.
As a practical matter, there is simply no reason that these types of traits should factor into admissions decisions. As a legal matter, awarding points for “cultural background” is likely a smokescreen for an attempt to reward candidates from racial groups “underrepresented in medicine.” In a notable exchange in the Supreme Court, a lawyer representing Students for Fair Admissions opined that it would be acceptable for colleges to reward students who write essays about dealing with cultural differences. In response, an incredulous Justice Kagan (who voted to uphold affirmative action) quipped: “The race is part of the culture and the culture is part of the race, isn’t it? I mean, that’s slicing the baloney awfully thin.”
Kagan isn’t necessarily correct to conflate race and culture. They are in fact distinct concepts, and it’s possible that VCU—for dubious reasons—aspires to reward applicants who, for example, were raised by cowboys in Texas or monks in the Himalayas.
However, it is clear that many across the healthcare establishment are searching for workarounds to the Court’s ruling against race conscious admissions, just as it is clear that VCU maintains a firm commitment to the DEI agenda. Against this backdrop, vigilance is needed to ensure that VCU sees matters differently from Justice Kagan and that race and culture are in fact treated as distinct concepts. Or, sensibly, the school could scrap the “diversity” component of their admissions process altogether in recognizing that it doesn’t predict physician quality but crowds out aptitude, work ethic and other traits that truly matter.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_41246344-1-scaled.jpg16672560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2024-06-21 19:37:562026-05-07 15:27:32VCU School of Medicine Highlights the Promise and Limitations of Affirmative Action Prohibition
Using official channels to oppose legislation raises serious institutional questions
Faculty at Dartmouth are using official institutional channels to rally student opposition to legislation that would classify individuals according to biological sex.
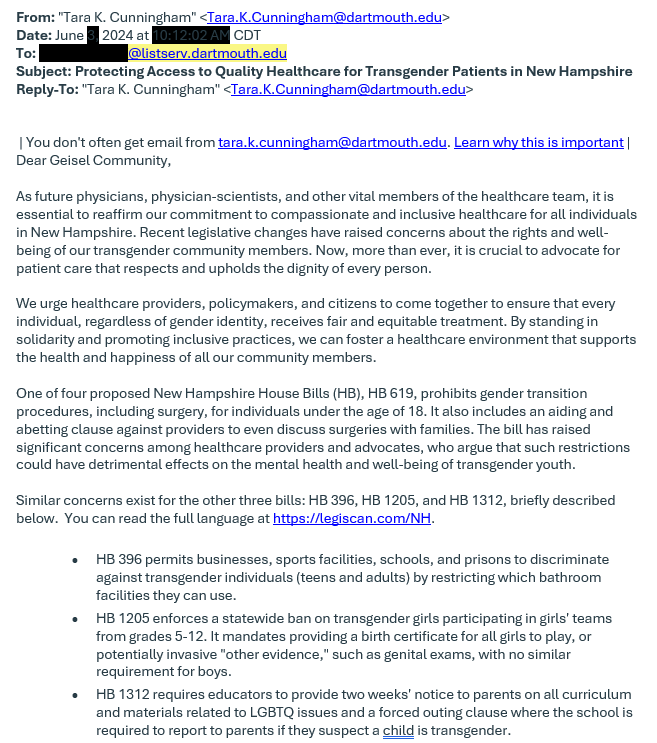
According to an email obtained by Do No Harm, faculty at Dartmouth’s Geisel School of Medicine are seeking to bolster student opposition to several bills advanced by the New Hampshire state legislature. “Recent legislative changes have raised concerns about the rights and well-being of our transgender community members,” wrote Tara Cunningham, associate dean for student life at Geisel, in an email from her official Dartmouth account to a student Listserv. “By standing in solidarity and promoting inclusive practices, we can foster a healthcare environment that supports the health and happiness of all our community members.”
Cunningham went on to urge students to contact New Hampshire Governor Chris Sununu and voice their opposition to the legislation. The bill, New Hampshire HB 619, would ban gender transition surgeries for children. Other legislation targeted in Cunningham’s email would require people at sports facilities, schools, and prisons to use the bathroom corresponding with their biological sex, ban biological males from competing in female sports teams in grades 5–12, and keep parents apprised of LGBTQ-related materials in schools. Such legislation would reinforce protections for students and children from being victimized in school or receiving irremediable sex reassignment surgeries while underage.
The completely justified premise of this legislation makes Dartmouth’s opposition even more concerning. The email to the student body also contained the signatures of Lisa McBride, Associate Dean for Diversity, Equity, Inclusion, and Belonging at the Geisel school, and medical student Nicholas An. It’s not entirely clear whether the email constitutes official guidance from the school, besides being sent from an associate dean’s school email to a official Dartmouth Listserv. No word on gender ideology has been forthcoming from Dartmouth president Sian Leah Beilock, herself the subject of recent controversy over having police remove a pro-Palestine encampment on Dartmouth’s campus.
If this opposition to defending biological sex is not representative of Dartmouth’s institutional position, the University ought to clarify this. Disagreement among faculty at a private university is a completely normal fixture of academic life and practice, but the use of official institutional channels to urge med students to advance gender ideology is a concerning development that Dartmouth ought to take seriously and explain.
The full text of the email from Cunningham, McBride, and An is below:
Figure 1. Email recently sent to students by Geisel School of Medicine associate deans.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_685959157-1-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2024-06-21 19:07:122026-05-07 15:28:56Dartmouth Dean Urges Students to Seek Lawmakers’ and Governor’s Defense of Gender Ideology
RICHMOND, VA, June 20, 2024 – Do No Harm filed a lawsuit against the discriminatory “Selected Professions Fellowships” program offered by the American Association of University Women (AAUW), which illegally excludes certain women based on race.
Women pursuing an education in one of AAUW’s designated degree programs can receive $20,000 and networking opportunities. Fellowships awarded for medicine, law, and business are “restricted to women of color” and are “open only to women from ethnic minority groups … Black or African American, Hispanic or Latino/a, American Indian or Alaska Native, Asian, and Native Hawaiian or Other Pacific Islander.”
AAUW’s “Selected Professions Fellowships” program violates the Civil Rights Act of 1866, 42 U.S.C. §1981, which requires racial equality in “to mak[ing] and enforce[ing] contracts.”
Do No Harm is filing on behalf of its medical-student members who meet all criteria laid out by AAUW but are ineligible to apply to the fellowship because of their race.
“We must keep identity politics out of medical education whether that be in the classroom or in medical fellowship programs,” said Dr. Stanley Goldfarb, Chairman of Do No Harm. “Every patient deserves access to the best possible care. Yet, ideologically driven fellowships such as those offered by the American Association of University Women, do not improve care. Medical fellowships should be awarded to students because of merit, not race.”
“The American Association of University Women should be ashamed of their archaic and illegal practice of discrimination based on race, said Kristina Rasmussen, Executive Director of Do No Harm. “As a women-led organization they should be lifting up all women. The AAUW should reverse course and open their fellowships and other opportunities to all women.”
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2024-06-20 15:57:072026-02-11 15:33:48Do No Harm Sues American Association of University Women for Racial Discrimination
Gov. Katie Hobbs has vetoed Arizona’s proposed Detransitioner Bill of Rights – a policy that aims to help young people hurt by a growing industry of medical practitioners and insurers that fund and perform gender transition surgeries on minors.
Mounting research suggests that so-called “gender affirming care” is harmful to children’s physical and mental health, with adverse health outcomes that threaten their wellbeing for the long term. To address this, a bipartisan group of leaders on the ground in Arizona sought recourse on behalf of these children and their families, many of whom are adults living with the adverse impacts of these ill-advised procedures being performed as children.
Chloe Cole, a victim and advocate on behalf of other gender-transitioned children and their families seeking accountability, responded to Gov. Hobbs’s veto:
“I have experienced first-hand the destruction that the gender transitioning industry can wreck on children. Our kids deserve to know that the same industry that abused them will be required to help them rebuild and restore their bodies. Clearly, Gov. Hobbs has a different agenda. Not only does her veto signal complete disregard for the children who have been preyed upon by this industry, but she also reveals her tacit support for the reputation Arizona is gaining as the nation’s emerging hub for the mutilation of minors. That may be a badge Gov. Hobbs is proud to wear, but I am confident that the vast majority of Arizonians will be deeply ashamed, as I am today.”
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2024-06-19 19:49:532026-02-11 15:33:48Do No Harm Comments on Arizona Governor’s Veto of the Detransitioner Bill of Rights
Like many other institutions, the American Board of Emergency Medicine (ABEM) accelerated its promotion of diversity, equity, and inclusion after the killing of George Floyd and its public statement on systemic racism in June of 2020.
Four years later, there is now little room left for debate within the organization.
In early 2022, ABEM’s Board of Directors declared diversity, equity, and inclusion a “strategic imperative.” A new committee on DEI was tasked with reviewing ABEM documentation, studying the perceptions of DEI among ABEM stakeholders, and working with external consultants to create new recommendations to advance DEI.
In July 2023, ABEM doubled down, issuing a revised Code of Professionalism that requires board-eligible and certified physicians to agree to “mitigate both implicit or explicit biases based on race, gender, age, sexual orientation, disability, national origin, or religion when providing patient care.”
Then, in November 2023, these efforts culminated in the Accreditation Council for Graduate Medical Education awarding the Barbara Ross-Lee, D.O., Diversity, Equity, and Inclusion Award to ABEM.
ABEM’s has transformed itself so rapidly that it has left little time or space for important questions about the foundations of its DEI policies. A major justification for DEI as an institutional priority was, for example, the claim by ABEM’s board of directors that diversity “leads to better patient care” served as a major justification for DEI as an institutional priority.
Of course, that claim is echoed by many other medical institutions, such as the American Association of Medical Colleges.
Yet, most of the evidence used to support the connection between race and patient outcomes does not actually evaluate outcomes, but perceptions of outcomes. This difference is subtly conceded by the AAMC. But even among studies that examine patient perceptions of outcomes based on the race of their doctors, the evidence is mixed.
Even the AAMC concedes the lack of evidence behind the claim that racial concordance between patients and doctors affects health outcomes: “that actual direct linkage… it’s not there.”
That concession, however, does not prevent AAMC, ABEM, or any other medical institution from continuing to spread misinformation about the link between the race of doctors and patient outcomes.
ABEM’s embrace of DEI and the lack of debate about its foundation are not unique. But the accelerated pace of change happening there serves as a cautionary example for other organizations that have not yet gone so far.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_146467091-1-scaled.jpg17212560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2024-06-17 18:46:352026-05-07 15:30:23American Board of Emergency Medicine Closed for Debate on DEI
DEI acolytes are loathe to let facts get in the way of narratives. Hopefully, students and faculty at the Virginia Commonwealth University (VCU) School of Medicine can spot the difference.
On May 30th, internal medicine grand rounds featured a lecture from Dr. Quinn Capers, a professor at the Howard University College of Medicine. The topic was “Diversity in Medicine: Battling the Anti-DEI Backlash with Data.”
Figure 1. VCU’s internal medicine grand rounds featured a lecture by Dr. Quinn Capers of the Howard University College of Medicine entitled “Diversity in Medicine: Battling the Anti-DEI Backlash with Data.”
Dr. Capers began with the question: “Why do we seek diversity in medicine?” He offered possible answers in a multiple choice format:
Underrepresented Minority Physicians Are More Likely to Serve the Undeserved.
Because Minority Patients Are More Likely to Follow the Recommendations of Minority Physicians.
Diversity on Research Teams Enhances Impact of Research
A Diverse Physician Workforce Will Reduce Racial Healthcare Disparities.
Ultimately, to the surprise of no one, Dr. Capers claimed “all of the above.” The evidence cited reveals more about how DEI steers medicine away from the pursuit of truth than anything else.
The first claim—that physicians from minority groups are more likely to serve minority or low-income populations—is true. However, the claim represents a solution in search of a problem.
Constraints on the supply of physicians are due to a limited number of seats in medical schools, not the number of people who aspire to practice medicine. There are thousands of highly qualified applicants rejected from medical school every year who would gladly work in urban or low-income communities.
The best hope for closing health disparities between different racial groups is to ensure that everyone has access to high-quality doctors, not recruiting individuals from specific identity groups to treat members of that group.
The second claim—that minority patients are more likely to follow the recommendations of minority physicians—is simply untrue. Dr. Capers references two studies to justify this idea. However, he conveniently ignores that a larger body of evidence contradicts the theory.
A lack of candor on the limitations of the two cherry-picked studies is also notable. The first (Saha & Beach, 2020) entails an experiment in which black and white patients with coronary artery disease view video vignettes in which a doctor recommends a coronary artery bypass graft (CABG). The study participants are randomly assigned to watch a vignette of a white doctor or a black doctor. Surveys administered right after the videos reveal that black patients who were assigned to watch the black doctor gave higher scores to the “perceived necessity of CABG” and the “likelihood of undergoing CABG.”
These findings represent tenuous evidence of the claim that minority patients follow the recommendations of minority physicians. It is well-documented that intentions reported on surveys are poorly predictive of behavior, including receipt of medical interventions. Respondents claiming that they are more likely to undergo CABG after watching a short video is a far cry from actually undergoing the procedure.
The other study (Alsan et al., 2019) referenced to plug the idea that minority patients follow the recommendations of minority doctors also offers tenuous evidence. The study consists of a two-part experiment. In the first part, black patients are shown a picture of a doctor and then surveyed about their willingness to undergo certain preventative health interventions.
Willingness to receive the treatments does not differ by the race of the doctor in the photo. Differences are only observed after the patients meet with the physicians. It wouldn’t be shocking if by random chance the six black doctors in the experiment happened to be more persuasive than the eight non-black doctors. It’s also possible that their persuasiveness was not coincidental. As the researchers admit, the doctors “could have inferred” that the study was about racial concordance and could have altered their behavior in response, a phenomenon known as a Hawthorne effect.
The third claim—that diversity on research teams enhances impact of research—is embellished. The authors of the paper cited by Capers (AlShebli et al., 2018) observe a correlation between research team diversity and the number of citations that papers receive. However, correlation is not causation, and there are confounding factors that more credibly explain the relationship. For example, liberals ascribe comparatively higher importance to racial diversity. That probably means, on average, racially diverse research teams produce research that more closely aligns with liberal orthodoxy and accrue more citations as a result.
Like the second claim, the fourth claim—that a diverse physician workforce will reduce racial healthcare disparities—is an assertion that relies on extreme cherry-picking. Dr. Capers cites one study—Snyder et al., 2023—to assert that black patients receive better care from black doctors. In fact, many studies address whether racial concordance is associated with improved outcomes, and those studied have been summarized across two systematic reviews published in the last five years, as Do No Harm documented, in a report on racial concordance in medicine. Systematic reviews are a useful mechanism to prevent cherry-picking and instead make sense of aggregated evidence. The two systematic reviews that touch upon racial concordance and outcomes emphatically reject a connection between them.
Figure 2. Among five systematic reviews on racial concordance, Otte and Zhao et al. specifically address outcomes.
The one study that Dr. Capers cites to justify the claim that black patients receive better care from black doctors purports to show that, at the county level, a higher proportion of black primary care providers is associated with a longer life expectancy for black residents and a reduction in the black-white mortality gap. The way that it derives a result at odds with other studies on racial concordance and outcomes is not difficult to decipher. There are a limitless number of arbitrary decisions that researchers make in developing mathematical models. For example, researchers must decide which variables to include, what time periods to observe, and which statistical techniques to use. Generally, researchers demonstrate that their findings would have been the same if they made different judgements about these things. Doing so shows readers that the researchers did not engage in p-hacking, a regrettably common practice whereby researchers try different model specifications until they find one that produces their preferred result. That the authors of this study did not demonstrate whether their findings are sensitive to model specification represents an enormous red flag.
Wherever it appears, DEI inevitably reveals itself to be an ideology at war with reason, facts, and logic. Medical students at VCU and across the country deserve better.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2149875605-1-scaled.jpg13502560supporthttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngsupport2024-06-13 18:29:542026-05-07 15:31:52VCU Grand Rounds Become Pulpit for DEI-Infused Misinformation
On June 12, 2024, Do No Harm Board Chairman Dr. Stanley Goldfarb submitted a comment on the Centers for Medicare and Medicaid Services’ (CMS) recently-proposed rule regarding the Increasing Organ Transplant Access (IOTA) Model, which will incentivize hospitals to create so-called “health equity” goals to reduce disparities in treatment for end-stage renal disease. If the rule takes effect, providers will almost certainly and intentionally select patients for kidney transplantation based on race. A more sensible solution—one focused on patient education—is possible and advisable.
In an effort to prevent CMS from encouraging such race-based practices with regards to kidney transplants, Dr. Goldfarb and Do No Harm are calling on CMS to withdraw its proposed rule.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2013632891-scaled.jpg13082560supporthttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngsupport2024-06-12 19:23:002026-05-07 13:20:18Do No Harm Calls on CMS to Withdraw Proposed Rule that Encourages Racial Prioritization for Kidney Transplants
Of course, the new report features all the usual talking points: DEI is good. Microaggressions are bad. Implicit bias training is necessary. And so on.
But there’s a twist this time. Buried in the report is an implicit – and occasionally explicit – admission that DEI training is not well-liked.
The Chronicle’s own data suggest that 47 percent of survey participants find it, at best “neither helpful nor unhelpful” or, at worst, “very/somewhat unhelpful”.
Figure 1. From the Chronicle of Higher Education’s “The Future of Diversity Training: Better Ways to Make Your College More Inclusive” report.
The authors of the report state that DEI training is good as long as no one speaks out against it or dares to express their concerns, which could “prompt people to avoid it, or even cause it to backfire.”
So, to recap, half of folks will either hate it or won’t get anything out of it. But you need to be trained. And it will be good – as long as nobody pushes back.
For their $8 billion per-year investment, the pro-DEI crowd isn’t getting much bang for their buck.
Another classic from the report: “Bad diversity training is worse than none at all.”
Really? Did the copy editor fall asleep?
At least good training makes a real difference though, right? Nope. Even the report acknowledges that the jury is out on DEI trainings, stating in clear terms that “A large body of research on the effectiveness of diversity training is inconclusive,” and “Some studies show that diversity training may actually backfire.”
The report goes on:
Diversity-training programs are now practically a rite of passage for college faculty and staff members, yet the evidence that they are effective is underwhelming…While there is a significant body of research on diversity training dating back decades, many studies rely on surveys that ask how participants felt about the training or assess what they’ve learned, while relatively few try to determine whether the training changed how people behave…The studies that do exist have found mixed results. Some show that participants learn about people from other backgrounds and that training can have an effect on beliefs and behaviors (although the latter fades over time). Others show that diversity-training programs can trigger negative feelings in participants and even harm the very groups they’re intended to help.
The Chronicle of Higher Education’s “The Future of Diversity Training: Better Ways to Make Your College More Inclusive” report
Critics of DEI could not have put it any better. Put simply, the report acknowledges the blatant failures of DEI up to this point, admits the lack of statistical rigor in many DEI evaluations, and showcases lackluster support for DEI.
One chart from the report even suggests that certain DEI trainings actually decrease diversity, with a 13.9 percent drop in black female managers following diversity trainings—a sharper decline than any other subgroup.
Figure 2. From the Chronicle of Higher Education’s “The Future of Diversity Training: Better Ways to Make Your College More Inclusive” report.
Yet, the report concludes that more DEI – even “bad” DEI – is the solution.
It is long-past time for the DEI industrial complex and higher education to take a long, hard look in the mirror.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1994910104-scaled.jpg17072560supporthttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngsupport2024-06-12 17:11:032026-05-07 13:19:12The Chronicle of Higher Education Admits it’s Easy to Hate DEI Training—and They’re Right
While campus administrators across the country continue to grapple with political protests, some of them violent and destructive, a more positive trend appears to be taking shape at two North Carolina universities with medical schools.
But with policymakers watching, how sincere is it? And how long will it last?
At least on paper, East Carolina University and the University of North Carolina are moving away from the divisive policies of the diversity, equity, and inclusion (DEI) culture toward strategies that instead emphasize a candidate’s academic competency and personal readiness for the rigors of medical school and, ultimately, a medical practice.
In the recent past, according to documents Do No Harm obtained through the Freedom of Information Act (FOIA), East Carolina University had injected DEI ideology into several aspects of its application process. For example, an interview question for applicants included as recently as 2022 was: “Name at least 3 ways in which classmates who differ from you in regard to their cultural, ethnic, religious, socioeconomic background, or sexual orientation could contribute to your development as a future physician.”
Even before the interview process, East Carolina’s screening guidelines in July 2022 gave points for life experiences and obstacles overcome such as discrimination, substance abuse, family violence, homelessness, or “mental issues with clear evidence of healing and recovery,” among other factors. Candidates also gained points for conducting research, demonstrating leadership, teamwork and service to others, as well as clinical experience. Those guidelines gave extra points for applicants who were underrepresented minorities, first-generation college students, and those who had “served minorities or marginalized populations.”
According to additional documents Do No Harm obtained, East Carolina has moved away from DEI. Now, interview questions cover situations involving compassion/empathy, responsibility/reliability, teamwork, and professionalism.
More publicly, the University of North Carolina-Chapel Hill is also taking positive steps. The Board of Trustees in May voted unanimously to redirect $2.3 million that funded DEI programs toward public safety initiatives on campus. “I think that DEI in a lot of people’s minds is divisiveness, exclusion and indoctrination,” trustee Marty Kotis told Chapel Hill-based public radio station WUNC.
Why the shift? For one thing, compliance with the June 2023 Supreme Court ruling ending affirmative action in education, based on the work of Students for Fair Admissions at Harvard College and the University of North Carolina, may be contributing to these changes.
Another factor is the potential for legislative efforts to prohibit DEI spending in public higher education. North Carolina would follow a number of other states including competitors Florida and Texas.
Under this microscope, North Carolina’s public university system is actively considering a policy to eliminate DEI system-wide.
The legislature seems content to watch and wait for now. And the public should encourage and embrace the state’s university system moving away from DEI on its own.
But members of the public and policymakers alike should regard any step in that direction with a healthy dose of skepticism unless and until a clear prohibition is codified into state law.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2264371317-scaled.jpg13502560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2024-05-28 20:08:032026-05-07 13:00:40North Carolina Schools Under the Microscope on DEI — What Will Legislators Do?
States across America are rolling back the pervasive influence that DEI has had in medical schools across the country. Some members of Congress, on the other hand, have rushed to its defense. And medical organizations have their backs.
Last month, five members of Congress introduced a resolution, H.Res.1180, entitled “Recognizing the importance of diversity, equity, and inclusion efforts in medical education.”
It contains the predictable platitudes. Among these are particularly dubious claims about racial concordance between providers and patients leading to better healthcare and the importance of DEI principles in medical education.
How many times must the disproven notion of racial concordance be disproven? Laymen and providers alike should understand that a patient’s access to high-quality care is far more predictive of health outcomes than access to care from providers of the same racial backgrounds. Increasing the quality of care and access to that care, not segregation, should be the priority.
And, of course, the resolution features the predictable contradiction that “discrimination, bias, and racism in medical education directly impacts the delivery of equitable health care throughout the United States,” as if DEI represents the repudiation, rather than the continuation, of discrimination, bias, and racism.
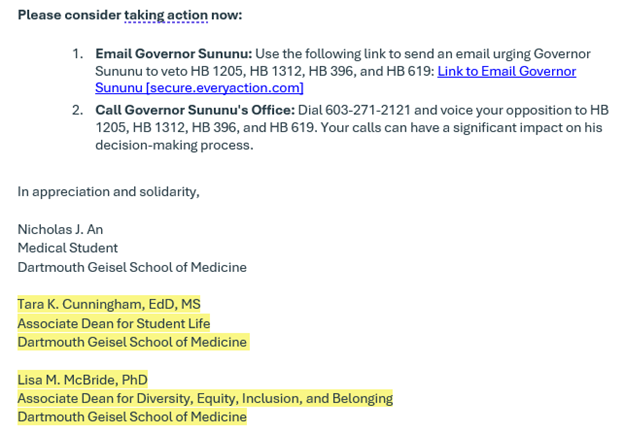
Concerned providers and members of the public have grown accustomed to virtue signaling and silly resolutions in Congress. But what might surprise some are the groups standing behind it.
Figure 1. From “e-Dear Colleague” email sent to members of Congress by Reps. Joyce Beatty and Kathy Castor on May 8, 2024.
More than two dozen major medical organizations in the United States have signed on to “endorse” this radical resolution. These include notable entities like the Association of American Medical Colleges (AAMC), the American College of Physicians (ACP), the American Association of Colleges of Osteopathic Medicine (AACOM), the American Society of Addiction Medicine (ASAM), and more.
This resolution has been referred to the House Committee on Energy and Commerce, where it is likely to remain in limbo for some time.
Indeed, several members of the committee have co-sponsored Rep. Greg Murphy’s EDUCATE Act, which would ban DEI in medical schools which receive federal funding. Of course, the AAMC and other medical organizations have lobbied against the EDUCATE Act.
Dues-paying individuals in these organizations would do well to remember what these groups stand for and do with their resources when asked to renew their membership. And policymakers unamused by this resolution and these medical organization’s pro-DEI stands should remember this moment when these organizations lobby for more power and money.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_634024823-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2024-05-24 18:26:002026-05-07 12:59:49Members of Congress Push Pro-DEI Resolution—And Medical Orgs Line Up Behind It
Policymakers and the public push back against DEI in the public square with increasing confidence. Why should the world’s leading medical journal be immune?
Enter Dr. Kathleen Brown, with a recent commentary submitted to the New England Journal of Medicine in response to an article published in March. That article was written by the American Medical Association’s “Chief Health Equity Officer,” Dr. Aletha Maybank. Among other things, it rebuked earlier efforts by Dr. Brown and colleagues to sunset DEI in dermatology, characterizing it as an assault on efforts to promote “equity” in medicine.
Figure 1. From the New England Journal of Medicine, March 20, 2024.
The New England Journal of Medicine, predictably, rejected Dr. Brown’s response. Of course, this makes it all the more worth reading:
In January 2024 I joined more than 80 other dermatologists in requesting that the American Academy of Dermatology sunset its DEI initiative. In a recent Perspective, Dr. Aletha Maybank rebuffed our concerns and warned that “eliminating DEI efforts negatively affects not only Black people, but all racially and religiously marginalized groups,” including “non-Christians.”
These assertions are emblematic of issues with DEI praxis. That is, dogma and politics are treated as substitutes for reason and evidence. There is no indication that DEI fosters harmonious group relations, but there is mounting concern that the reductive “oppressor/oppressed” paradigm regularly adopted by DEI advocates shelters and instigates antisemitism. Indeed, the many Jewish doctors agitating for change in dermatology would plainly disagree that DEI efforts are “rooted in values of belonging.”
Meaningful debate about DEI has rightly reached the public square. I hope the American healthcare system is allowed to follow suit and that TheNew England Journal of Medicine plays a leading role in fostering constructive dialogue.
Kathleen Brown, M.D., member of the American Academy of Dermatology.
As Dr. Brown writes, there is no evidence that DEI improves patient care or outcomes and good reason to suspect the opposite. Similarly, there is no evidence that DEI fosters inclusivity in medicine, but ample evidence that it shelters and instigates hostility against Jews.
A medical journal interested in the dispassionate, apolitical pursuit of truth would recognize these shortcomings and allow open debate about the merits of an ideology that manifests in medical recruitment, training, research, and practice. Unfortunately, the New England Journal of Medicine is too ideologically committed to racial separatism to take on that role.
We salute Dr. Brown for her efforts to engage in fruitful debate about DEI. Judges, policymakers, and members of the public are listening, even if the editors of this once esteemed journal aren’t.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1686925927-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2024-05-24 12:11:202026-05-07 12:59:00New England Journal of Medicine Brooks No Dissent of DEI
When it comes to virtue signaling, the Medical University of South Carolina (MUSC) spares no expense.
On January 1, 2024, Dr. Michael de Arellano became MUSC’s new chief equity officer. In his official duties, he leads the Office of Equity team and “is responsible for ongoing and new efforts to promote a culture of equity, eliminate disparities, and foster an inclusive environment for students, faculty, staff, and patients.”
Documents obtained from MUSC by Do No Harm via a Freedom of Information Act (FOIA) request indicate that Dr. de Arellano will be paid a base compensation of $370,000 annually. But that’s just his base salary. He has the potential for “executive variable compensation” of 5%, 10%, or 15%. The Department of Psychiatry will fund $50,000 of Dr. de Arellano’s base compensation for his clinical role.
Additionally, Dr. de Arellano was due to be paid a $20,000 bonus within 30 days of his start date, as well as a $20,000 bonus for completing his “onboarding goals.”
Figure 1. Unconscious Bias Advisory Council at MUSC.
[Perhaps de Arellano’s first order of business will be asking MUSC to practice what they preach, given that the university’s Board of Trustees is comprised of over 80 percent white males—hardly a model for the diversity they claim to embody.]
MUSC joins a lamentable club of public universities that pay DEI staff exponentially more than their full-time tenured professors. Unfortunately, this is not a new phenomenon, as seen in a March 2022 article on Fox News. Speaking on behalf of the Heritage Foundation, Do No Harm senior fellow Jay Greene stated that DEI on campuses creates a “political orthodoxy, which fundamentally distorts the intellectual and political life on campus.”
But perhaps MUSC’s willingness to spend so much on a DEI hire is unsurprising, given the university’s blatant use of DEI criteria in its admissions process. For example, admissions interviews include screening for “cultural competency” and “cultural experiences/diversity”, with an evaluation scale for “cultural awareness”. An extra rubric provided to evaluate applicants gives up to 20 points based on candidates scoring on a “Cultural Experiences/DEI Efforts” scale. And interviewers are not even provided applicant GPAs or MCAT scores, in order to protect the process from “implicit bias”.
However, the school places a great deal of emphasis on GPA and MCAT in the information it provides to prospective applicants. They are told that they must have a GPA of at least 3.5 and a minimum MCAT score of 506 to apply or to be considered for an invitation to complete a secondary application – below the averages that MUSC claimed during the 2023-2024 admissions cycle.
Figure 2. From “Applying to Medical School” (MUSC Office of Admissions).
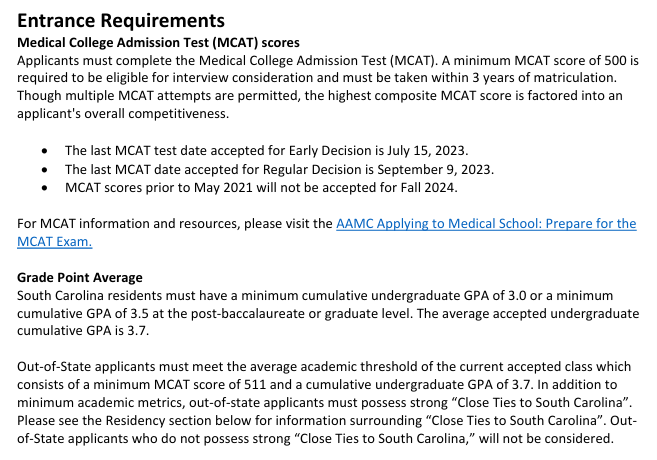
Yet, the same document notes that “to be eligible for interview consideration,” the MCAT minimum is 500 and the minimum GPA is 3.0 for South Carolina residents.
Figure 3. Entrance Requirements from “Applying to Medical School” (MUSC Office of Admissions).
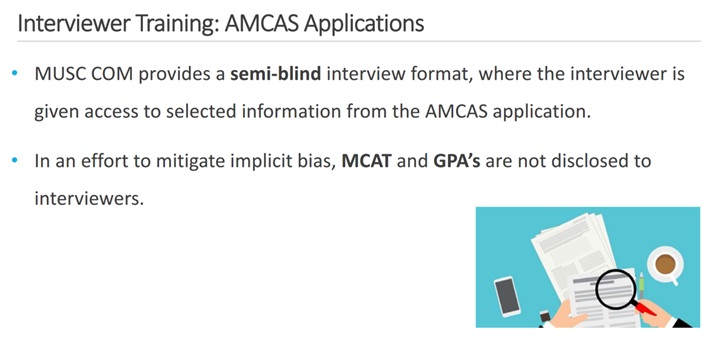
Members of the MUSC College of Medicine (COM) faculty and staff who conduct applicant interviews were provided with training by the College of Medicine Office of Admissions. Learners are reminded of the COM mission to foster “a diverse educational community” to “promote the equitable health and well-being” of South Carolina residents. Interestingly, the training notes that American Medical College Application Service (AMCAS) applications, managed by the Association of American Medical Colleges (AAMC), “are semi-blind for all reviewers.” Interviewers are “given access to selected information from the AMCAS application.” In addition to the academic minimums and residency requirements, interviewers are instructed to use metrics with “potential for added value.” Topping that list is “Cultural and DEI efforts.”
Figure 4. “COM Office of Admissions Interviewer Training: 2023-2024 Cycle” at MUSC (slide 14).
The slides listing the “attributes” to consider and structured questions to evaluate them were redacted.
At a time when public colleges and universities in several states are dissolving their DEI offices, MUSC is demonstrating its dedication to divisive concepts in the name of “health equity” – with no credible evidence to support their effectiveness. And, despite the Supreme Court’s ruling making affirmative action in college admissions illegal, MUSC is among the schools that are sticking to the AAMC’s “holistic admissions” agenda to skirt the Court’s decision.
South Carolina taxpayers must ask why their tax dollars are going toward funding such an initiative at MUSC, and look to their neighbors to the north for inspiration on how to restore merit as the cornerstone of medical education.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2155407549-scaled.jpg13502560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2024-05-23 10:26:342026-05-07 12:57:12The Medical University of South Carolina Drops $370K on a Chief Equity Officer – And Shows Its Obsession With All Things DEI
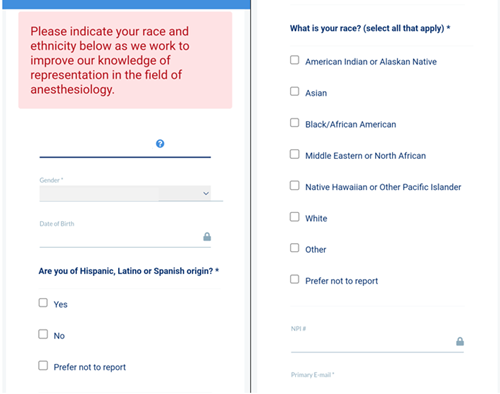
First, you will need to decide whether or not to declare your race and ethnicity.
Think you can bypass it? Think again. While a “Prefer not to report” choice exists, the site displays a red-letter announcement to “Please indicate your race and ethnicity below as we work to improve our knowledge of representation in the field of anesthesiology.”
Why?
Figure 1. Login screen to the ABA member website.
Why are ABA members being prompted to choose a racial group before they can access their services? Like all physicians, anesthesiologists need to complete ongoing education to maintain their board certification. Their employment depends on it.
Why must physicians who have already taken an oath to “do no harm” and treat all patients with the utmost care and dignity give yet another organization data that could be to be distorted in service of racist DEI efforts?
To its credit, the ABA does note in its 2024 Policy Book that data on “gender, race, and ethnicity” is collected on members. This reflects a continuation of a revision made to the Winter 2023 Policy Book, section 7.11: Data Privacy and Security Policy.
Figure 2. ABA Winter 2023 Policy Book Changes document, page 4.Figure 3. ABA 2024 Policy Book, page 53.
But, again, why? Elsewhere in the Policy Book, it simply states that data can be collected “to conduct research.” But a press release is more revealing, explaining the organization’s decision to collect private ethnicity data on their candidates so “that we are properly supporting” people.
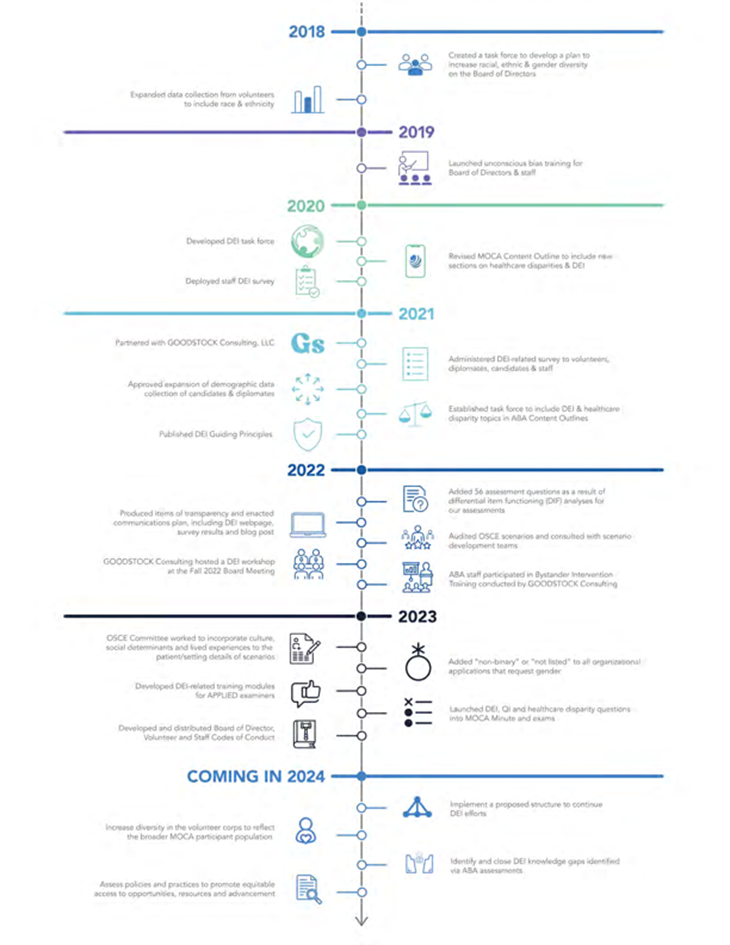
At this point, individuals familiar with today’s equity jargon know that such language is far from innocuous. And the public jargon is clearly having an impact behind the scenes. The ABA proudly highlights it DEI efforts, posting a timeline of changes over the years, including developing a DEI taskforce in 2020.
Figure 4. “ABA DEI Timeline” from the ABA website (click here for expanded view).
According to the timeline, the ABA is taking steps to “increase[e] diversity” in the organization’s volunteer corps and reassessing “policies and practices to promote equitable access to opportunities, resources, and advancement.”
Here’s an alternative path forward: focus on competence, not color. Patients understand this. Professional medical organizations should too.
As Kingbury and Greene noted, “attempts to match patients to doctors on the basis of race hold no promise for producing better care or better outcomes.” And medical institutions should always put health outcomes for patients above placating activists and furthering race-based preferences.
To that end, almost one year has passed since the Supreme Court struck down affirmative action programs in higher education as constitutional violation. A growing number of states have prohibited public funding for DEI programs. The tide is turning.
Yet, racial classifications continue to play a role at the ABA and for anesthesiologists seeking to obtain and maintain board certifications. Why? And when will it end?
Do No Harm believes in making healthcare better for all – not undermining it in the pursuit of a political agenda or identity politics. Do No Harm seeks to highlight and counteract these divisive trends in medicine.
https://donoharmmedicine.org/wp-content/uploads/2024/05/shutterstock_2083979461-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2024-05-20 06:19:002026-02-11 15:33:47The American Board of Anesthesiology Prods Members to Declare Race and Ethnicity When Accessing Online Services
Ohio University Heritage College of Osteopathic Medicine (OUHCOM) has discontinued its Physician Diversity Scholars (PDS) Program (archived page here) as the result of a federal civil rights investigation by the Department of Education’s Office for Civil Rights (OCR).
As we reported last December, OUHCOM was partnering with the Cleveland Clinic to offer the program, which was “open to all underrepresented minority medical students.” The school defined “underrepresented minority” as “Black/African-American, Hispanic/Latino, Native American/Alaskan Native and pacific Islander/Native Hawaiian,” in violation of Title VI of the Civil Rights Act of 1964.
Following the complaint (filed by Do No Harm Senior Fellow Mark Perry) and subsequent federal investigation, OUHCOM has discontinued the discriminatory program and replaced it with the Brentwood Foundation Community Physician Scholars Program – free of race-based eligibility criteria.
Figure 1. Landing page of the Brentwood Foundation Community Physician Scholars Program.
“The Scholars Program takes a proactive approach to building diversity by giving students who have experienced socioeconomic, educational, or other disadvantages a unique opportunity for growth and engagement,” the updated program landing page states.
The Cleveland OCR issued an investigation closure notice on May 13, 2024, citing that OUHCOM had discontinued the PDS program and stopped promoting the program on its website, and verified the new program “does not include any eligibility or participation criteria restricted by race or national origin.”
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2012352206-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2024-05-17 12:53:002026-05-07 12:56:10Ohio University Scraps a Discriminatory Program Following a Federal Civil Rights Investigation
Race-based mandates may sound like long-abandoned antiquities of the pre-civil rights era. But one organization purporting to represent family medicine wants to roll back the clock.
In an email anonymously shared with Do No Harm, the Association of Family Medicine Residency Directors (AFMRD) details that they are “deeply concerned” regarding the “erasure” of Diversity, Equity, and Inclusion (DEI) in medical institutions. What is that erasure? Recent legislative efforts across the country to defend equal treatment regardless of race. The email points to thirty pending bills which would “dismantle” DEI initiatives and specifically highlights seven anti-DEI bills that have been signed into law, as well as the federal EDUCATE Act.
Figure 1. From a May 7, 2024 email sent to AFMRD members.
These bills should be a cause for celebration. States like Florida,Utah,Texas, and more have worked to curtail the influence of DEI in colleges and universities (including medical institutions of higher education). These meaningful reforms protect students and faculty from loyalty oaths, mandatory diversity trainings, and other discriminatory policies. Meanwhile, the EDUCATE Act, sponsored by Congressman Greg Murphy of North Carolina, would rightly cut off federal funding to medical schools’ DEI programs.
But rather than celebrate these successes, the AFMRD is up in arms. In its latest email, the organization is urging members to take matters into their own hands by contacting legislators and taking to social media using the “#diversity” as the hashtag.
One of the resources linked in the AFMRD’s email is to the Society of Teachers of Family Medicine (STFM) and their “Family Medicine DEI Advocacy Toolkit”. This so-called “toolkit” includes a map tracking these “deeply concerning” pieces of legislation, links to an online “advocacy course”, social media graphics, and more.
Figure 2. From the STFM Family Medicine DEI Advocacy Toolkit landing page.
STFM also decries the EDUCATE Act, noting that the act would “ban race-based mandates at medical schools and accrediting institutions”—as if ending racist quotas and policies would harm healthcare instead of helping it.
These organizations are hardly the first entities to embrace divisive DEI concepts. From osteopathic medicine to psychiatry, organizations representing members in countless medical subfields have embraced identity politics in healthcare at the expense of individual merit and evidence-based healthcare.
However, the AFMRD and STFM’s call to political action to salvage DEI in medicine represents a much deeper commitment.
What if these medical organizations actually focused on, say, medicine? What progress could be made with this time and energy if it were devoted to research, evaluations of new practices, or moral and ethical considerations?
It is difficult to comprehend how, in the 21st century, it is controversial to claim that racial discrimination in medicine is a bad idea. But it is.
The sooner these organizations are called out for their clearly harmful views and actions, the better it will be for medical providers and patients alike.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1747491581-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2024-05-15 20:44:212026-05-07 12:54:51Who Supports Race-Based Mandates? As It Turns Out, Family Medicine Organizations
Medical schools and organizations have made defiant statements against the Supreme Court’s ban on race-based admissions
Richmond, VA; May 15, 2024 – Prestigious medical schools continue to discriminate based on race and are committed to continue to find work arounds to the Supreme Court’s ruling in Students for Fair Admissions v. Harvard and Students for Fair Admissions v. North Carolina are the findings in a report released today by Do No Harm.
The report reveals prestigious medical schools such as Stanford made defiant statements in wake of the ruling: “Stanford Medicine firmly believes in the transformative power of diversity, in all dimensions… While the ruling changes the landscape of university admissions, it does not change our resolve or our values. We reaffirm that commitment to you today and in the days to come.”
In addition to Stanford, leading medical organizations also were dissatisfied with the court curtailing their political agenda. The report warns the Association of American Medical Colleges (AAMC), a group with a track record of forcing progressive political agendas into the accreditation process, could attempt to compel medical schools to follow the AAMC’s politized DEI standards.
“Abolishing DEI at medical schools is also instrumental in redirecting admissions committees toward merit and aptitude rather than identity politics. DEI corrupts all facets of academic life and compels a fixation on group representation, including within the admissions process.” said Dr. Stanley Goldfarb, Chairman of Do No Harm.
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. With more than 7,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and in 14 countries, DNH has achieved more than 7,800 media hits in top-tier publications and garnered widespread attention through numerous broadcast news appearances.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2024-05-15 15:07:002026-02-11 15:33:47Do No Harm Releases Report Exposing Medical Schools for Skirting SCOTUS Ruling
Ohio State University (OSU) is up to its same old tricks, living up to its nickname as a “Destination for Indoctrination.” OSU hosted a DEI conference on May 6 and 7 for The National Conference on Diversity, Race & Learning (NCDRL).
NCDRL explains that “the conference offers a multi-leveled examination of ‘diversity’ as a concept and its implementation within institutions of higher education, the corporate world, the religious community, [and] the larger community, including public service.”
Instead of genuinely bridging “the economic, political and socio-educational divides that continue to be pertinent in the American social landscape and beyond,” as is the stated goal, OSU’s Office of Diversity and Inclusion pushes divisive ideology on faculty and students.
The conference’s registration page warns that the event is already as “maximum capacity,” having convinced a full house of attendees to pay between $250-$460 each. It also appears that OSU may have paid employees to attend or, at least, on their behalf given that W9 tax forms were provided for payment.
Figure 1: The National Conference on Diversity, Race & Learning at Ohio State University.
The title of the conference is “What’s Next? Equity in a Changing World.” But the real question is what’s next for Ohio in a changing nation as smart states crack down on DEI? Ohio’s flagship university continues to deepen its commitment to woke indoctrination without pushback from policymakers.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1884285844-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2024-05-14 17:29:382026-05-07 12:53:43Maximum Capacity: DEI Conference an Expensive Reminder that Ohio Tolerates Woke Propaganda in Public Universities
In the wake of the Supreme Court’s ruling which prohibits race-conscious college admissions, is West Virginia University School of Medicine following the law? Maybe. But materials included in an admissions committee training workshop raise serious questions. And the school’s leadership owes applicants, lawmakers, and the public clear answers.
The training slideshow, obtained by Do No Harm through a public records request, offers mixed signals about the school’s understanding of the Court’s decision in Students for Fair Admissions v. Harvard (2023). In summarizing the decision, a slide first notes that applicants “must be treated based on his or her experiences as an individual – not on the basis of race.” This is, of course, true. However, it goes on to claim that race is considered “as one factor among many, in an effort to assemble a student body that is diverse in ways broader than race.”
Figure 1. From “2023 Committee on Admissions Training Workshop,” WVU School of Medicine.
This language can be traced to a different Supreme Court ruling, Grutter v. Bollinger (2003), the very decision that SFFA explicitly overruled. And that most recent ruling made it clear: Race can’t be a factor in the admissions process at all.
Other slides suggest that the admissions committee understands the Court’s decision and intends to comply with it. For example, the updated diversity policy removes references to race-conscious admissions and instead affirms a focus on selecting “a diverse student body, faculty, and staff, including the socioeconomically disadvantaged rural Appalachian population.”
Figure 2. From “2023 Committee on Admissions Training Workshop,” WVU School of Medicine.
Previously, in 2022, the policy stated that “the School endeavors to select a gender-balanced and diverse student body, faculty, and staff including underrepresented in medicine groups, including those who identify as African-American, Hispanic, and Native American/Pacific Islander.”
Figure 3. From “2023 Committee on Admissions Training Workshop,” WVU School of Medicine.
Hopefully the attribution of a quote from Bollinger to SFFA is an honest mistake and the admissions committee understands that race-conscious admissions are a violation of the Fourteenth Amendment’s Equal Protection Clause. Either way, WVU has some explaining to do.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2373313565-scaled.jpg19202560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2024-05-13 14:59:092026-05-07 12:52:10WVU Has Some Explaining To Do