During its 47th Annual Refresher Course in Family Medicine, the University of Pittsburgh Medical Center hosted a March 6 session, titled “Racial Health Disparities” and presented by Stephanie Miller, MD and Kristina Johnson, MD.
The session was replete with political advocacy and references to DEI, critical race theory, and implicit bias.
For instance, Johnson spent a significant portion of the discussion going on a diatribe against the public health policies of the Trump administration.
“There is an ongoing attempt at erasure of trans people. There are outright attacks on gender affirming care,” Johnson said. “Immigration and Customs Enforcement has ended its policy of staying out of healthcare facilities, and the Department of Education may be cutting financial support for students with disabilities. As physicians, we must speak up. Use your voice.”
Without delving too deeply into the political nature of these attacks, it’s worth noting that the Trump administration’s actions regarding so-called “gender-affirming care” have only been to restrict federal funding of such interventions for children.
Moreover, in addition to citing founder of critical race theory Richard Delgado, Miller called for healthcare professionals to engage in active anti-racism, using an example of a moving walkway at an airport.
“Actively racist behavior is equivalent to walking fast on the conveyor belt. Passive racist behavior is equivalent to standing still on the walkway. No overt effort is being made, but the conveyor belt moves the bystanders along to the same destination as those who are actively walking. Some of the bystanders may feel the motion of the conveyor belt, see the active racists ahead of them, and choose to turn around; but unless they are walking actively in the opposite direction at a speed faster than the conveyor belt, unless they are actively anti-racist, they will find themselves carried along with others.”
Anti-racism in practice often holds that racial discrimination is praiseworthy and necessary. It seeks to overcome different outcomes among racial and gender groups by actively discriminating in favor of some people and against others. Its most famous advocate, Ibram X. Kendi, made his embrace of racial discrimination explicit: “The only remedy to past discrimination is present discrimination. The only remedy to present discrimination is future discrimination.”
At another point in the discussion, Miller talked about how to practice this ideological form of medicine in practice.
“You can provide gender-affirming care by confirming that you’re using your patients’ or your colleagues’ correct names and pronouns,” Miller said. “You can use ancestry rather than race to describe the risk of disease.”
Additionally, at various points in the discussion, both Miller and Johnson dismissed the idea that health disparities between racial groups could be explained by physical/genetic differences.
Johnson summarizes her point succinctly here:
“We have talked about how the social construct of race was used by white people to gain and hold onto power, and how that resulted in health disparities between races; and the false conclusion that those disparities are based in genetics rather than racism. We’ve also explained that racism is anything that increases the disparity between racial groups, whether that’s intentional or not; and we use this narrow focus because the historical path and present-day disparities are so glaringly obvious.”
This is misleading. For instance, as our own Director of Research Ian Kingsbury has shownusing the example of preeclampsia, in which about 55 percentof risk is estimated to be genetic, “West African ancestry is linked to risk variants in a gene called alipoprotein L1 (APOL1) that dramatically increase the likelihood of developing preeclampsia or kidney disease.” Genetic differences obviously play a role in numerous other conditions.
In other words, genetic differences between different groups of people obviously lead to differences in particular health outcomes, and it is dangerous to dismiss this fact.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2273908799-1-scaled.jpg14402560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-03-26 13:13:352026-05-11 13:55:03University of Pittsburgh Medical Center Hosts Political Activists, Advocates of Critical Race Theory
Earlier this month, Stanford University offered a continuing medical education course in the form of a webinar titled “The Supreme Court’s 2023 Affirmative Action Ruling: What Does it Mean for Health Equity and Public Health?”
Speaking at the course was Dr. Michelle A. Williams, the former Dean of the Faculty at the Harvard T.H. Chan School of Public Health.
Williams offered a full-throated defense of racially discriminatory policies and criticized the Supreme Court’s decision in Students for Fair Admissions v. Harvard (which found racially conscious admissions illegal), justifying her arguments in the name of diversity and equity.
Particularly revealing was the language used by Williams to characterize the impact of this decision, and the regime she instead wished remained in place.
“Our conclusion was that the focus on racial neutrality was flawed,” Williams said.
Additionally, Williams mourned the ostensible negative effects of the Supreme Court’s decision, arguing that the lack of an ability to racially discriminate will impair healthcare.
“Medically underserved areas are going to be even less well served as a result of the workforce shortages,” Williams said. “There will continue to be a reduced ability to provide culturally competent care, affecting the quality of healthcare across diverse communities.”
Williams then proceeded to make several seemingly incorrect claims.
“We also know from emerging literature and well done studies concordant care, meaning the aligning of care with social and cultural status, leads to better health outcomes for marginalized populations and that concordant care can increase patient experience, can improve screening, which will improve preventive measures…and we’ve seen that mortality rates for black newborns for example, dropping by half when black physicians care for the patients,” Williams said.
It’s not clear what study exactly Williams is referring to, but her claim does bear a striking similarity to a false claim by Supreme Court Justice Ketanji Brown Jackson, which stated that “for high-risk black newborns, having a black physician more than doubles the likelihood that the baby will live.”
Justice Jackson’s claim is incorrect for a number of statistical reasons; but beyond that, the famous study often used to support racial concordance on the basis of improving black infant mortality is methodologically flawed.
Proponents of DEI and race-conscious admissions in medical schools have frequently cited the 2020 study, “Physician–patient racial concordance and disparities in birthing mortality for newborns,” to argue that medical schools should prioritize race in admissions in order to increase diversity among physicians and thereby improve care for minority patients. The 2020 study examined Florida infant mortality data and purported to show that the elevated infant mortality rate among black babies was partially reduced when black babies had black doctors rather than white doctors.
But a 2024 commentary published in the same journal, examined the same data and found that, when controlling for very low birth weights, the racial concordance effect becomes statistically insignificant in the most comprehensive statistical models that include hospital and physician fixed effects.
Moreover, Williams’ general point about the positive effects of racial concordance are similarly incorrect.
Do No Harm’s report on racial concordance highlighted the fact that four out of five systematic reviews found no evidence to support the claim that racial concordance improves health outcomes. Moreover, the fifth systematic review suffered from methodological flaws, such as the unexplained omission of studies that contradicted its conclusion.
Williams then went on to provide recommendations for how schools can continue to pursue these diversity and equity goals.
“Staying within…the framework of our laws, the strategic acts that would be necessarily [sic] to counteract the decline in our healthcare workforce that is represented in our population would require us to continue to look for ways to expand how we do our admissions processes to be holistic,” Williams said. “Holistic means looking at socioeconomic factors, as well as the life experiences, along with the academic metrics of applicants.”
Although it’s not clear what decision-making process Williams has in mind, as Do No Harm has shown holistic admissions is often a proxy for racially conscious admissions; it provides a veneer of plausible deniability for medical schools to continue to consider race in their admissions decisions while devaluing objective metrics like MCAT scores and GPAs.
Williams then suggested scholarships for “diverse” students as a way to continue addressing health equity.
“Financial support is going to be important, particularly providing scholarships for…students of diverse backgrounds, particularly of low socioeconomic strata,” Williams said.
It’s worth noting that restricting access to scholarships on the basis of race is illegal; Do No Harm has filed numerous complaintsagainst medical schools that offer racially discriminatory scholarships.
In sum, this course amounts to a defense of racially discriminatory admissions policies and a eulogy for racial discrimination.
Needless to say, these ideas have no place in medical education, and are antithetical to the principles of merit and excellence that serve as the foundation of medical practice.
And in light of the Supreme Court’s decision, such ideas are illegal and should be confined to the dustbin of history.
https://donoharmmedicine.org/wp-content/uploads/2025/03/videoframe_2902162.png7201280Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-03-26 12:55:222026-02-11 15:34:01Harvard Professor Mourns Death of Racially Discriminatory Admissions in CME Course
This week, Republican lawmakers in Oregon sent a letter to Attorney General Pam Bondi correcting false claims made in a lawsuit against the Trump administration.
The letter comes in response to claims made in a lawsuit by several Democrat-run states over a recent executive order curtailing federal funding to providers of child sex changes; Oregon is one of the states suing the Trump administration over the order.
In their complaint, the states make the claim “that transgender minors do not receive gender-affirming genital surgery.”
As Do No Harm Visiting Fellow Paul Terdal demonstrated in National Review earlier this month, this is blatantly false:
In 2021, the Oregon Health Authority provided me with a copy of its insurance claims database for the year 2019. The database covers the private health insurance and Medicaid payments for all medical procedures of 92 percent of the state’s population. This includes gender-affirming treatment. In 2019, two biological girls had their ovaries and uteruses removed because of their gender distress. They were just 17 years old. Four 18-year-olds also received genital surgeries.
Moreover, according to insurance claims data obtained by Do No Harm, there were 26 genital surgeries performed on minors between 2019 and 2023. Additionally, 330 minors received “top” surgeries such as breast reductions or double mastectomies.
The letter from the Oregon lawmakers further requests a federal investigation into Oregon’s use of Medicaid funds; the lawmakers accuse the Oregon Health Authority of “concealing the extent of taxpayer-funded procedures on minors and suppressing internal findings that show no evidence of benefit.”
This is in reference to a review of the “evidence” supporting child sex change procedures by the Oregon Health Authority’s Health Evidence Review Commission, which found a “paucity of data” and no systematic reviews to show the benefits of these interventions. However, the report was never published; instead, the commissioners endorsed guidelines from the radical activist group WPATH, or World Professional Association for Transgender Health.
“This is state-sponsored medical experimentation on kids, paid for with your tax dollars,” said Representative Ed Diehl, one of the lawmakers behind the letter. “The DOJ needs to act—this isn’t health care, it’s political ideology.”
Do No Harm applauds this effort to correct the record. As we’ve seen over the past few years, advocates of so-called “gender-affirming care” are not abovemaking false or misleading claims to support their agenda.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_249441406-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-03-26 12:47:092026-05-11 13:53:45Oregon Lawmakers Set the Record Straight on Child Sex Changes
Earlier this week, Do No Harm filed a civil rights complaint against Geisinger College of Health Sciences (GCOHS) in Pennsylvania over its discriminatory DEI programs.
GCOHS, by its own admission, prioritizes “the recruitment and inclusion of … traditionally underrepresented minorities in medicine and biomedical sciences, specifically African American/Blacks, Latinos/Hispanics and Native Americans as members of [its] faculty, staff, and student body.”
The Geisinger Commonwealth School of Medicine also used a $3.4 million federal grant toestablish a “Center of Excellence for Diversity and Inclusion.” The Center’s primary goal has been described as building “a leakless pipeline to expand the pool of underrepresented-in-medicine (URM) candidates” for medical school admission and faculty positions.
The offending programs mentioned in our complaint mirror GCOHS’s institutional posture regarding DEI and political activism.
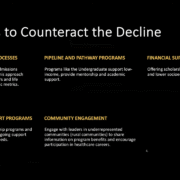
Do No Harm obtained a presentation for GCOHS administrators that highlighted“challenges” facing the school today.
These challenges include “ICE activity” and changes to “DEI initiatives” and “gender-affirming care.”
Figure 1. A slide from a GCOHS presentation.
First, it’s not clear what federal immigration policies or the Trump administration’s ICE activity have to do with the mission of a medical school. The notion that these issues would be an area of concern indicates that GCOHS’s priorities extend into the political realm.
Second, the school’s listing of DEI initiatives reflects just how much these programs matter to GCOHS.
It’s also worth noting that “gender-affirming care” is grouped under the DEI category.
These DEI priorities are also reflected in Geisinger’s Strategic Plan for 2023-2028; the plan includes a commitment to “continue to diversify college faculty, staff and learners to better serve our communities.”
Geisinger also aims for its “academic components [to be] aligned with system goals, adding value to the system mission and enhancing effectiveness of assets in areas of shared concern such as DEI, well-being, professionalism, and leadership development.”
It’s clear that GCOHS has a deep institutional commitment to DEI.
We hope that it takes our complaint to heart, abandons its DEI endeavors, and instead focuses on the true mission of medical schools: teaching the practice of medicine.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1214860510-1-scaled.jpg12802560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-03-24 19:49:542026-05-11 13:52:10Geisinger College Makes Clear Its Commitment to Radical Activism
DEI activists insist that racial/ethnic group differences in academic readiness for medical school or performance in medical school must be evidence of racist systems. In response to this imagined racism, they demand reform that obfuscates differentiation in performance. So, for example, “holistic admissions” tone down the once-prominent role of MCAT scores and GPA in determining medical school admission in favor of fuzzy personal attributes, like the candidate’s commitment to the school’s mission.
Because “underrepresented” (i.e. black or Hispanic) applicants tend to have significantly lower GPAs and MCAT scoresthan white and Asian applicants, this enables medical schools to continue advancing their diversity goals with plausible deniability that they are engaging in racial discrimination.
The latest absurdity comes from University of Texas Medical Branch researchers publishing in the journal Advances in Medical Education and Practice. The studysupposedly “aims to compare traditional admissions interviews with Multiple Mini Interviews [i.e. 7 to 9 short interviews instead of one long one] to assess their reliability in evaluating applicants across racial and socioeconomic backgrounds.” The data for this study comes from the University of Texas Medical Branch John Sealy School of Medicine (JSSOM), which changed its interview format to mini interviews in 2022 after the “admissions committee observed inconsistencies in interview scoring, topics discussed during interviews, and interviewer comments using an unstructured interview format.”
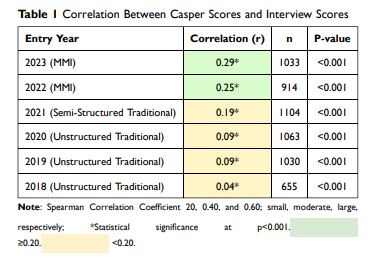
The “study” involves two separate analyses. In the first part, the researchers observe the correlation between interview scores and Casper scores according to interview type. “The Altus Assessments Casper test is an online situational judgment test designed to evaluate an applicant’s noncognitive skills, including ethical judgment, communication, and professionalism.” The correlation between interview score and Casper score improves from essentially non-existent to small when the school adopts multiple mini interviews.
Figure 1. A table showing the correlation between interview scores and Casper scores.
At face value, this would seem to speak well to the multiple mini interviews format. In reality, however, there is no test that can accurately assess “an applicant’s noncognitive skills, including ethical judgment, communication, and professionalism.” Were that so, all employers would be administering these tests to prospective employees. Instead, these types of skills are appraised as a matter of human judgement. In the case of medical school, it’s likely that they are best evaluated through long interviews that test a candidate’s endurance and limit their ability to offer scripted answers. In other words, the multiple mini interview format is a solution in search of a problem.
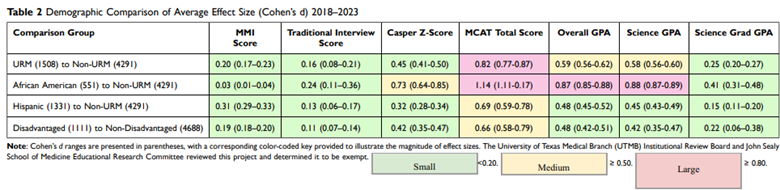
In the second part of the analysis, the researchers assess whether using the multiple mini interview format reduces ethnic and economic group differences in interview score. They observed that multiple mini interviews “reduced differences compared with traditional interviews for African American candidates and slightly increased differences for URM, Hispanic, and disadvantaged candidates.” Of course, group differences in interview scores are no more evidence of discrimination than differences in MCAT scores, but the researchers don’t entertain that reality and favor an orthodoxy that differences must be evidence of discrimination.
In a particularly revealing display of their motives, the researchers show group differences in MCAT scores and GPAs but provide the information in a convoluted way that makes it impossible for the reader to discern which groups perform higher.
Figure 2. A table showing group differences in MCAT scores and GPAs.
Again, generally speaking, applicants from groups “underrepresented in medicine” (i.e. Hispanic and black) have significantly lower GPAs and MCAT scoresthan white and Asian applicants and face lower admissions standards. Acknowledgement of this fact is made all but impossible by their rationalization that multiple mini interviews allow “for a more granular and specific evaluation of candidate abilities, improving the precision of scoring by reducing subjectivity and enhancing reliability in assessing key competencies.” A test like the MCAT is the gold standard when it comes to “objectivity.” Were that indeed their primary concern, they would conclude that, on average, candidate quality does in fact vary by ethnic group.
Ultimately, it’s unclear whether multiple mini interviews facilitate skirting the Supreme Court’s ruling against affirmative action. What is clear, however, is that tinkering with the admissions process at JSSOM is occurring in service of racial consciousness. As the researchers themselves acknowledge, “Finding a way to assess the interpersonal and intrapersonal characteristics of applicants accurately is critical given the recent Supreme Court decisions in Students for Fair Admissions, Inc. (SFFA) v. University of North Carolina and SFFA v. President & Fellows of Harvard College.”
JSSOM, like all schools, should be focused on attracting the beat and brightest candidates. This study should invite healthy skepticism regarding the school’s commitment to that principle.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2269385773-1-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-03-24 12:07:372026-05-11 13:49:05University of Texas Medical Branch ‘Study’ Hints That the School Remains Fixated on Race
The New England Journal of Medicine (NEJM)is distributing a 14-question survey to healthcare organizations regarding their opinions and experiences pertaining to “structural racism.”
The survey includes questions inquiring as to the prevalence of structural racism in a provider’s organization, how structural racism impacts “care delivery,” tactics utilized in addressing structural racism, the deployment of DEI-related metrics, the presence of a safe space to discuss DEI-related concepts, and much more.
The NEJM makes clear its preferences: that healthcare organizations should treat racial groups differently in order to promote “diversity.”
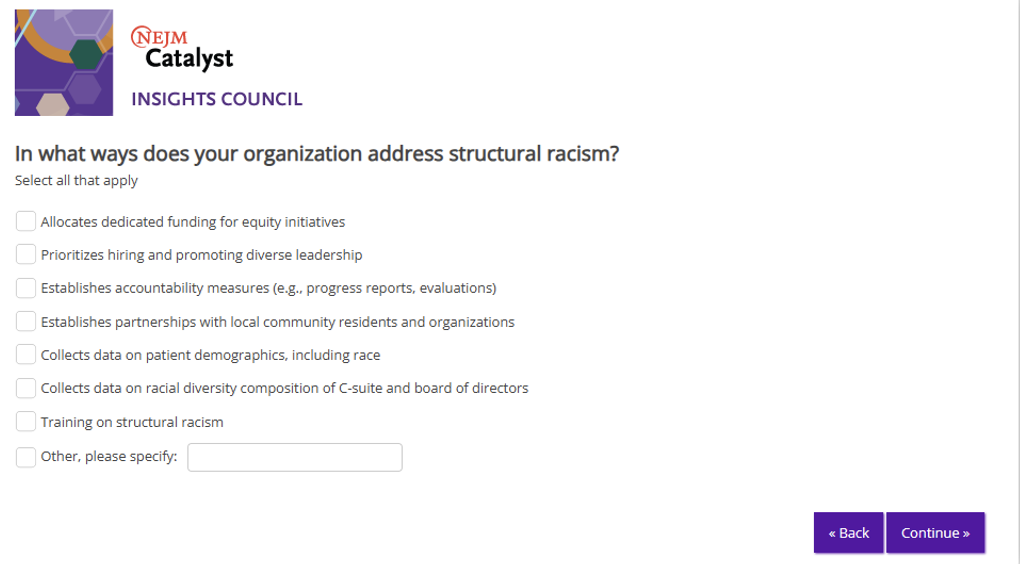
For example, NEJM gives several options for organizations to “address” structural racism when asking how organizations currently go about doing so. Several of the options provided in this multiple choice question relate to intertwining personnel decisions with racial criteria, including “prioritizes hiring and promoting diverse leadership” and “collects data on racial composition of C-suite and board of directors.”
Figure 1. A question from the NEJM survey.
This type of racial-quota-focused hiring is regressive and obviously detrimental to a healthcare organization’s mission to actually, you know, provide healthcare, so it’s disappointing to see this behavior encouraged by such a “respectable” publication.
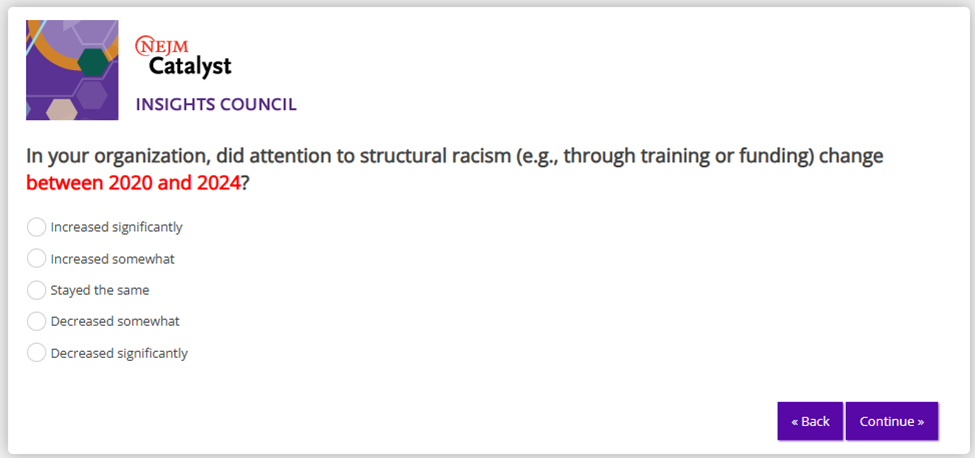
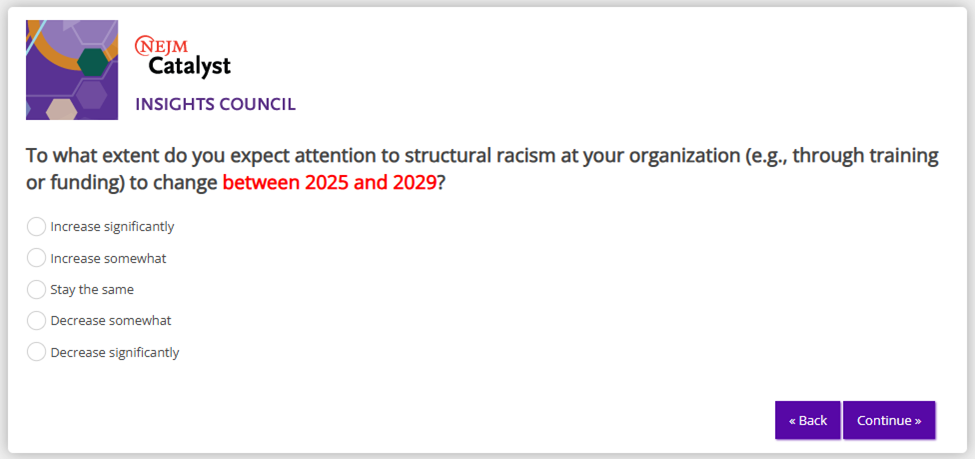
The survey further asks respondents to assess their organization’s commitment to address structural racism, thereby giving the NEJM a metric to determine how committed to “the cause” the referenced organizations truly are.
Figure 2. A question from the NEJM survey.Figure 3. A question from the NEJM survey.Figure 4. A question from the NEJM survey.
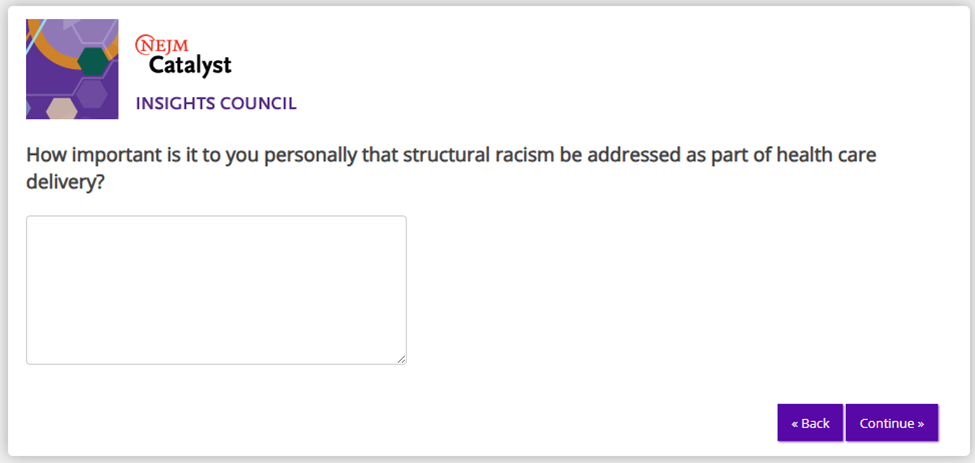
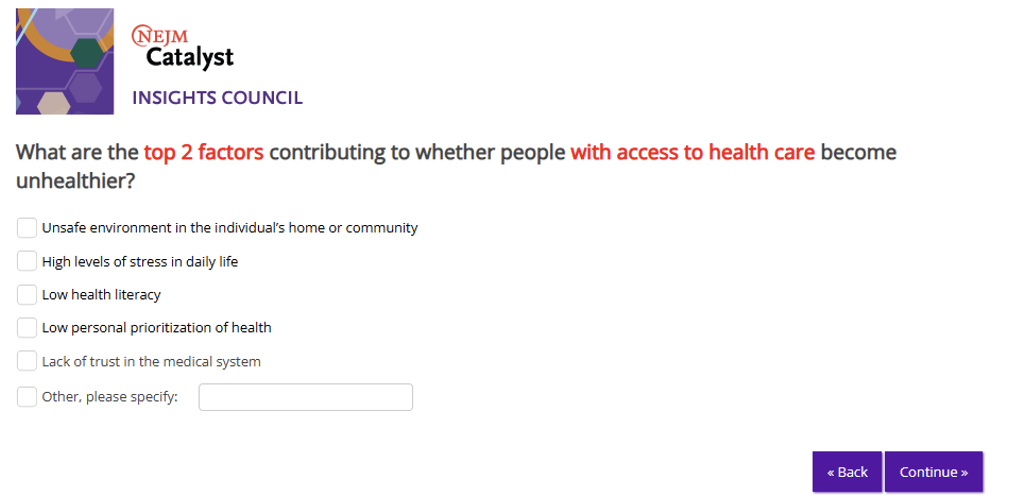
Additionally, some of the questions and prompts appear to be an ideological screening test; for example, after asking several questions about the relationship between structural racism and care, NEJM poses the question “What are the top 2 factors contributing to whether people with access to health care become unhealthier?”
Among the options provided as answers are unsafe environments, stress, low health literacy, low prioritization of health, lack of trust in the medical system, and other.
Figure 5. A question from the NEJM survey.
The NEJM has a long history of this behavior; in May 2023, Do No Harm organized a petition condemning NEJM’s publication of an articlecalling for explicit racial discrimination in medical education. The petition garnered the support of more than 1,000 health care professionals across a wide range of subfields.
A different article published by NEJM called for doctors to practice “anti-racist documentation” while another characterized “racism” as the chief culprit behind most health disparities.
And after one doctor submitted a commentary pieceto NEJM in response to an article by the American Medical Association’s Chief Health Equity Officer, the Journal rejected the response.
What purpose will NEJM’s latest survey serve? That remains to be seen. But based on the presence of multiple questions at the end of the survey asking participants for their permission to use their responses for their “Insights Report,” one can make a reasonable guess.
The Virginia Commonwealth University – and its affiliated medical institutions VCU Health and VCU School of Medicine – are no strangers to DEI. VCU Health advertises its DEI programs on its website, while the medical school toutsits commitment to DEI.
Yet it’s clear DEI has pervaded these institutions even deeper.
In fact, according to documents obtained by Do No Harm, almost 400 VCU Medical Center job descriptions contain references to “diversity.”
This includes references to diversity in the position’s desired qualifications and duties.
For instance, the job description for the Vice President and Chief Medical Officer of Health System Transformation requires candidates to have a “demonstrated ability to leverage diversity in functional skills, experience levels and backgrounds for innovation.”
The Chief Medical Officer role states that candidates should have a “Diversity Equity and Inclusion certification.”
A human resources position states that candidates are responsible for recruiting “historically underrepresented” populations.
VCU’s institutional commitment to DEI is further evidenced in a grand rounds session that has since gone viral.
Fox News reported that during the grand rounds session, Dr. Haywood Brown, associate vice president of Academic Affairs at the University of South Florida (USF), made a number of incendiary comments about how medical school faculty and administrators could skirt Florida’s anti-DEI laws.
🚨 BREAKING – In explosive leaked audio, top @USFHealth official Haywood Brown, MD, reveals how he is evading anti-DEI laws – and teaches doctors how to evade them as well.
“We no longer have a person who's dedicated to [diversity]. We have a council that's dedicated to it.… pic.twitter.com/oydHZfqVQd
Following Fox News’ report, Brown resigned from his position at USF.
But attendees, including VCU professor David Chelmow, applauded Brown, with Chelmow calling his speech “wonderful.”
But that’s not all; Do No Harm also obtained documents from theVCU Massey Cancer Centerrevealing VCU’s DEI education programs.
The documents include lesson plans and descriptions of “Advanced Research Mentoring Programs” operated by the VCU School of Medicine as a form of education that “provide evidence-based practices and techniques for research faculty to grow and hone their mentoring.”
Thelesson plan for the initial ARM session is essentially entirely focused on DEI.
Activity titles include “Reflecting on Diversity,” “Reflect on Unconscious Assumptions,” “Implications of Diversity Research,” and “Case Studies,” with the latter discussing examples of, you guessed it, “Equity and Inclusion.”
According to theprogram description of an ARM session, the sessions are designed to help faculty “recognize the potential impact of conscious and unconscious assumptions, preconceptions, biases, and prejudices on the mentor-mentee relationship and reflect on how to manage them.”
Do No Harm also obtained the slide deck for one of the ARM sessions that includes, among other references to DEI, the infamous cartoon depicting “equity,” featured below.
Figure 1. A photo demonstrating “equity” from a VCU educational slide deck.
“Equity is about giving everyone what they individually need to be able to participate/see what is happening/do research (ex. Having a lab bench at the height someone would need if they used a wheelchair),” the slide deck notes state.
Additionally, the slides note that the session involves an eight minute-long exploration of DEI research; another ARM document includes a list of studies ostensibly demonstrating examples of prejudice against racial minorities.
Do No Harm has previously documented VCU’s commitment to DEI and racially discriminatory ideology.
For instance, 2024 admissions guidelines obtained by Do No Harm from the VCU School of Medicine revealed that the school continues to reward “diversity” in the admissions process.
Additionally, VCU School of Medicine hosted a lecture featuring several flat-out misleading claims such as: “Underrepresented Minority Physicians Are More Likely to Serve the Underserved,” “Minority Patients Are More Likely to Follow the Recommendations of Minority Physicians,” “Diversity on Research Teams Enhances Impact of Research,” and “A Diverse Physician Workforce Will Reduce Racial Healthcare Disparities.”
https://donoharmmedicine.org/wp-content/uploads/2025/03/image-e1742408780697.png479844Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-03-19 18:25:302026-02-11 15:34:01VCU Health’s DEI Problem
RICHMOND, VA; March 19, 2025 – Today,Do No Harm submitted two complaints to the U.S. Department of Health and Human Services (HHS) Office for Civil Rights (OCR) against Duke University Health System (DUHS) and Geisinger College of Health Sciences (GCOHS).
The complaints identify several instances in which DUHS and GCOHS engaged in unlawful race-based discrimination in their programs and policies.
For instance, DUHS’s diversity plan explicitly calls for adapting admissions processes to increase acceptance of underrepresented minority applicants, even pairing prospective minority candidates with current minority students to “create community and a sense of belonging” during the admissions process through a “holistic review.” Internal DUHS documents tout deliberate admissions decisions to boost enrollment of certain racial groups.
GCOHS, by its own admission, prioritizes “the recruitment and inclusion of … traditionally underrepresented minorities in medicine and biomedical sciences, specifically African American/Blacks, Latinos/Hispanics and Native Americans as members of [its] faculty, staff, and student body.” GCOHS also used a $3.4 million federal grant to establish a “Center of Excellence for Diversity and Inclusion.” The Center’s primary goal has been described as building “a leakless pipeline to expand the pool of underrepresented-in-medicine (URM) candidates” for medical school admission and faculty positions.
“Medical schools like Duke and Geisinger continue to flout the idea of colorblind recruitment, merit-based admissions, and equal opportunity enrichment programs, despite a clear directive from the highest court in the land. Their actions are just another example of how DEI ideology has infiltrated every facet of American medicine,” said Dr. Kurt Miceli, Medical Director of Do No Harm. “Schools and health systems cannot be allowed to continue these obviously discriminatory practices, especially when they have the vital job of producing our future doctors. Relying on intrinsic characteristics – and not merit – undermines the very principle of equal opportunity and ultimately puts patients at risk. It is both illegal and immoral. Duke and Geisinger must be held accountable.”
Read the complaint against Duke University Health System (DUHS) here and the complaint against Geisinger College of Health Sciences (GCOHS) here.
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. With 16,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 14 countries, DNH has achieved over 10,000 media hits in top-tier publications and garnered widespread attention through numerous broadcast news appearances.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-03-19 18:20:212026-02-11 15:34:01Do No Harm Files Civil Rights Complaints Against Duke University Health System and Geisinger College of Health Sciences
Editor’s note: This blog post was initially submitted as a Comment to JAMA Network Open in response to the article, “Race-Specific and Race-Neutral Equations for Lung Function and Asthma Diagnosis in Black Children.” JAMA rejected our submission.
In their article “Race-Specific and Race-Neutral Equations for Lung Function and Asthma Diagnosis in Black Children,” Chang, et al. (2025)tacitly dismiss the possibility that variation in lung capacity by race could have a biological explanation. They’re mistaken. Harik-Khan, Muller and Wise (2004)observed that “socioeconomic, nutritional, and environmental variables” only explain 7–10% of the difference between black and white children vis-à-vis lung volume. Even when factoring in anthropometric factors the researchers could only explain half of the difference in lung volume. Stocks, Sonnappa and Lum (2014) also concluded that “African genes are associated with lower lung volumes.”
Furthermore, asthma is diagnosed based on clinical history and evidence of variability in expiratory airflow obstruction. Static measurement of forced expiratory volume exhaled in 1 second (FEV1), whether using a race-neutral or race-specific equation, is grossly inadequate to detect asthma, as shown by the poor sensitivity and specificity of the test for either black or white children.
Taking the Cincinnati Childhood Allergy and Air Pollution Study (CCAAPS) data presented in Chang, et al.’s article, the sensitivity and specificity using the race-specific equation for percent predicted FEV1 in black children were 18.2% and 81.3%, respectively. Using the race-neutral formula, sensitivity improved to 72.7%, but at the expense of specificity falling to 42.9%. In other words, the new, race-neutral equation missed fewer black children with asthma, but at the cost of misdiagnosing more black children with asthma who don’t actually have the disease.
For white children in this dataset, the percent predicted FEV1 using the race-specific equation was similarly poor at 31.8%. Specificity was 85.1%. Using the race-neutral formula, sensitivity fell to 24.2%, while specificity remained relatively unchanged at 86.4%. Effectively, use of the race-neutral equation made a lousy result even worse for white children. The same pattern is seen in the Mechanisms of Progression from Atopic Dermatitis to Asthma (MPAACH) data, which the article also references.
The author’s conclusion of “structural racism” is unfortunately misplaced and divisive. As Witonsky, et al. (2022)noted, “spirometry could benefit from reference equations that incorporate genetic ancestry.” Moreover, predicted FEV1 is inadequate to detect asthma in both black and white children no matter the formula used. Rather than hunt for alleged “outdated racist practices” research should focus on truly improving the clinical diagnosis of asthma for all people.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2447034123-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-03-19 11:47:422026-05-11 13:48:29Use of Race in Pulmonary Function Tests Isn’t Racist
RICHMOND, VA; March 18, 2025 – Today, Do No Harm filed a lawsuit against Penn Medicine, the Consortium of DEI Health Educators, and WURD Radio for their discriminatory physician directory that excludes doctors based on race.
Penn Medicine, the Consortium of DEI Health Educators, and WURD Radio operate the Black Doctors Directory, an advertising and marketing opportunity provided exclusively to black doctors in southeastern Pennsylvania, New Jersey, and Delaware. Non-black doctors are excluded from the Directory regardless of how regularly they treat black patients or how much they have worked to improve black patients’ health.
The Directory is founded on the false premise that racial concordance, in which patients are treated by physicians of the same race, improves health outcomes. This ideology sows distrust between doctors and patients. Do No Harm has debunked this false belief in its report, Racial Concordance in Medicine: The Return of Segregation.
The Directory violates Title VI of the Civil Rights Act of 1964 as well as Section 1557 of the Affordable Care Act, which bans racial discrimination in federally funded health programs.
Do No Harm is filing the lawsuit on behalf of one of its members who is excluded from the Directory based on race, even though they regularly treat black patients in southeastern Pennsylvania.
“The Black Doctors Directory is yet another example of Penn Medicine and other institutions prioritizing identity politics over care,” said Stanley Goldfarb, MD, Chairman of Do No Harm. “It is both wrong and a gross misuse of taxpayer money to exclude doctors from the Directory’s advertising advantages just because they are not black. Furthermore, the Directory’s foundational claim that racial concordance produces better health outcomes has been thoroughly debunked. If Penn Medicine and others wants to improve health outcomes for patients, then it would advertise and recommend the highest quality doctors, regardless of their race.”
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. With 16,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 14 countries, DNH has achieved over 10,000 media hits in top-tier publications and garnered widespread attention through numerous broadcast news appearances.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-03-18 21:04:062026-02-11 15:34:01Do No Harm Files Lawsuit Against Penn Medicine for Discriminatory Directory
RICHMOND, VA; March 18, 2025 – Today, Do No Harm published a report titled, “Unethical Expectations: How Accreditors Inject Identity Politics into Medical and Healthcare Education.” The report highlights 10 accreditors for medical and healthcare education that impose DEI requirements and/or reference the value of “diversity” in their accreditation standards.
These standards range from explicitly requiring DEI offices to indirectly encouraging diversity-related outcomes.
The 10 offending accreditors include:
The Liaison Committee on Medical Education
Accreditation Council for Pharmacy Education
American Association of Colleges of Nursing
American Osteopathic Association Commission on Osteopathic College Accreditation
American Dental Association Commission on Dental Accreditation
American Podiatric Medical Association Council on Podiatric Medical Accreditation
Accreditation Council on Optometric Education
Commission on Accreditation in Physical Therapy Education
American Psychological Association Commission on Accreditation
American Veterinary Medical Association Council on Education
For instance, the American Osteopathic Association’s Commission on Osteopathic College Accreditation (COCA) standards, which set requirements for osteopathic medical education programs that grant Doctor of Osteopathic Medicine (DO) degrees, explicitly require dedicated DEI programs and offices for colleges of osteopathic medicine (COMs) to be accredited.
“Our new report shines a much-needed light on the all-powerful actors in healthcare education,” said Dr. Kurt Miceli, Medical Director at Do No Harm. “Wielding unchecked control, accreditors have long had the ability to force member institutions to comply with their standards. Over the past decade, their shift toward political and social activism has furthered the imposition of DEI requirements on these graduate medical and healthcare education programs. Applicants, students, and patients are now paying the price. If these governing bodies want to earn back the public’s trust, they must depoliticize their standards and focus on prioritizing expertise and high-quality care in the institutions they accredit.”
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. With 16,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 14 countries, DNH has achieved over 10,000 media hits in top-tier publications and garnered widespread attention through numerous broadcast news appearances.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-03-18 12:32:172026-02-11 15:34:00New Do No Harm Report Reveals How Accreditors Inject DEI Into Medicine
RICHMOND, VA; March 17, 2025 – This month, Do No Harm launched our newsletter, “Youth Gender Medicine Today,” a new resource highlighting the current state of play in the field of pediatric gender medicine.
The Spring 2025 edition of the newsletter, sent to Do No Harm members, providers of gender-related medical services, and other stakeholders in the medical community, identifies trends in medicine and society at large demonstrating how the country is turning away from the “gender affirmation” approach to pediatric gender medicine.
Now, more than ever, it’s important to highlight the current trends that demonstrate the tide is turning against the child transgender industry. This newsletter provides a comprehensive analysis of the current state of pediatric gender medicine from the perspective of medical experts and advocates working to protect our country’s children.
“Times are changing. The more the evidence behind so-called ‘gender-affirming care’ is scrutinized, the more the child transgender industry is discredited,” said Stanley Goldfarb, MD, Chairman of Do No Harm. “Do No Harm is doing our part to ensure that our members within the medical community understand this fact.”
To join Do No Harm and support our efforts to restore trust and scientific rigor in medicine, sign up here.
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. With 16,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 14 countries, DNH has achieved over 10,000 media hits in top-tier publications and garnered widespread attention through numerous broadcast news appearances.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-03-17 18:57:462026-02-11 15:34:00Do No Harm Launches First-of-Its-Kind Newsletter Highlighting State of Gender Medicine
Last month, Dr. Lisa Cooper, the director of the Johns Hopkins Center for Health Equity, appeared on an episode of the Johns Hopkins School of Public Health podcast to defend the DEI movement and its underlying ideology.
The episode, titled “The Concepts Behind The Language of Equity,” is framed as a response to – and a means of explaining – the “backlash” to DEI over the past few years.
In it, Cooper attempts to spin DEI as simply a misunderstood and well-intentioned effort to help everyone; the language of “race” and “racism” are downplayed and in their place are references to nebulous concepts like “needs” and “backgrounds.”
“I think one thing that people oftentimes get confused about is that they think we are aiming for equality; which is a good thing, you know, to be fair and give everyone the same thing but, in order to achieve health equity, which is on the other side of the coin from health disparities, you have to give people what they need,” Cooper said. “And not everyone starts from the same place, or has the same needs.”
When placed in the context of race, this is just an indirect way of describing racial discrimination. If one is “giving” individuals different things based on their “needs,” and those needs are determined by race, then one is discriminating.
Cooper then tries to redefine “diversity” without its racial connotation.
“There’s this whole phrase that’s been created – DEI terminology – that I guess is supposed to mean something that’s negative,” Cooper said. “But in reality, diversity basically just means having people from different backgrounds, and different ways of thinking, and different life experiences, and making sure we appreciate that, which I think is a basic American value.”
This is not what diversity means “in reality” – the term in practice refers to racially discriminatory practices and policies. Diversity scholarships reward certain racial groups over others; diversity in the student body entails discriminatory admissionspolicies.
In fact, Johns Hopkins’ own DEI initiatives discriminate against certain racial groups.
Do No Harm has shined a spotlighton Johns Hopkins before, running an advertising campaign exposing its discriminatory behavior after Dr. Sherita Hill Golden, the former chief diversity officer for Johns Hopkins Medicine, sent out a memo labeling white males and Christians as possessing innate “privilege.” Golden resigned shortly after.
In January, we filed a civil rights complaint against Johns Hopkins after the university restricted access to certain programs to medical students from racial groups deemed to be “underrepresented” in medicine.
Cooper goes on to argue that the consequences of DEI are that “no one is left behind or disadvantaged.”
But DEI, by its very nature, disadvantages certain racial groups while favoring others.
At the end of the day, this spin doesn’t change the underlying reality that DEI in practice amounts to racial discrimination.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_221825779-1-scaled.jpg17062560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-03-17 14:39:192026-05-11 13:47:22Johns Hopkins Plays Dumb in Defense of DEI
A recent article by Chris Rufo and Hannah Grossman of the Manhattan Institute offers an unflattering profile of Dr. Jennifer Manly, a neuropsychologist and Columbia professor. Manly is an agitator within the pro-Hamas campus movement. Her activism spills into her research, much of it based on “the so-called social determinants of health thesis, which posits that racism, sexism, and homophobia can cause brain disease in ‘Black and Latinx communities.’”
Rufo and Grossman note that critics have described the thesis as “pseudo-science.” Manly and her defenders would surely disagree, pointing to her impressive collection of scholarly publications and citations. However, peer review in medical journals is often just as much a screen for ideology as it is one for rigor. A careful examination of a study that Manly recently co-authored makes for a useful illustration of just how faulty this line of research is, and why it is incumbent upon the NIH to stop funding it.
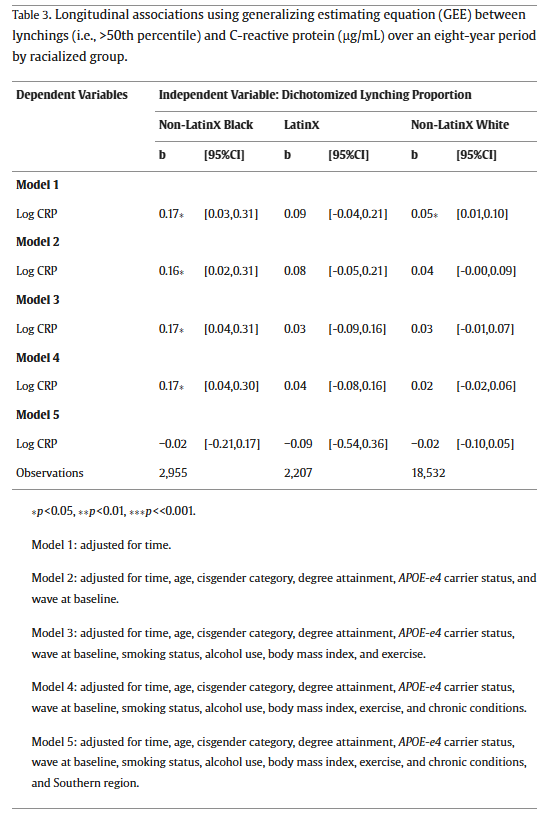
The study, “’Rest of the folks are tired and weary’: The impact of historical lynchings on biological and cognitive health for older adults racialized as Black,” was published in the journal, Social Science & Medicine, by ten authors, with Manly’s name appearing last.
From Social Science and Medicine, January 2025.
As the title suggests, the study examines the effect of lynchings on health outcomes. It claims to find that residing in states that historically had more lynchings of black victims causes black subjects to experience a greater increase in a measure of inflammation and a greater decline in cognitive function. The theory it offers to account for these findings is that experiencing lynchings activates a “stress response in early childhood” that contributes to adverse health outcomes later in life.
The article only supports this claim by using a convoluted and indefensible research design and by interpreting the results in implausible ways. Rather than devising a measure of lynching that might capture the likelihood that one was exposed to lynchings, they discard information and dichotomize the 37 states that had any lynchings of black people into having above median or below median number of lynchings. As they describe it, “we dichotomized the variable at the 50th percentile (median), where less than the median corresponded to states with 1 lynching and greater than the median corresponded to states that had 2 or more lynchings.”
As one of many examples of sloppiness, the median number of black victims of lynchings among the 37 states with at least one lynching is 16, not 1 or 2. And the median among all 44 states in the Tuskegee Institute’s data set is 5. Another egregious example of sloppiness is that the article mis-describes the Emancipation Proclamation as having been issued in 1864, when it was actually issued onJanuary 1, 1863. And in another error, the text describes the main result inconsistently with how it is described in the tables. [i]
Regardless of how the researchers divided states into above and below median lynching categories, dichotomizing the data threw away information that prevented a more fine-grained examination of the health effects of lynchings. The effect of living in Mississippi, which had 539 black victims of lynchings between 1882 and1968, is treated the same as living in Virginia, with 83 lynchings, or Illinois, with 19. All would be above median, however they calculated it.
The researchers make no adjustment for the population of states, so that California, with 2 black victims of lynching, is treated the same as Montana, which also has 2. If the researchers are hoping to measure exposure to lynching, failing to differentiate between the size of states is a serious shortcoming.
But the most serious failure of the study is that the results of its fully specified model do not find that health outcomes are worse among black subjects in states classified as having a higher number of historic lynchings. As can be seen in Model 5 of Table 3, being in a state with above median historic lynchings is not significantly related to the CRP measure of inflammation among black subjects.
From “’Rest of the folks are tired and weary’: The impact of historical lynchings on biological and cognitive health for older adults racialized as Black.”
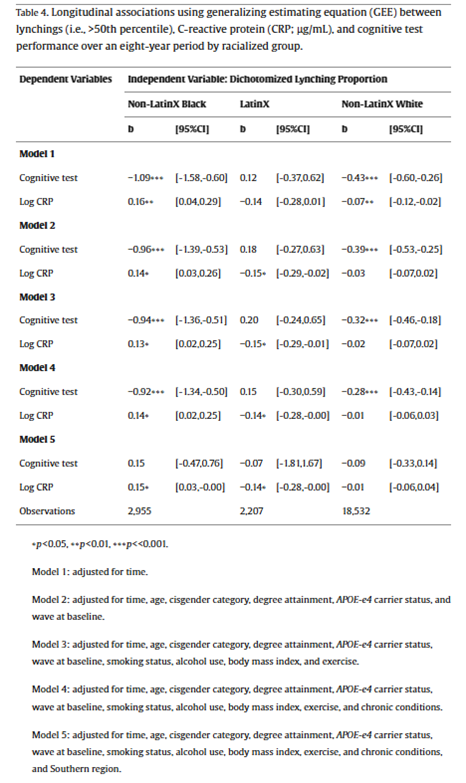
And in Model 5 of Table 4, residing in a state with an above median number of historic lynchings is not significantly related to the measure of cognitive performance among black subjects.
From “’Rest of the folks are tired and weary’: The impact of historical lynchings on biological and cognitive health for older adults racialized as Black.”
In model 5, the researchers add to their set of controls a variable for whether the state is in the Census definition of the South. So, what their research really shows is that black subjects who live in the South have worsening measures of inflammation and cognitive performance, not that historic lynchings contribute to adverse health outcomes. That is, within the South, being in a state that had above or below median numbers of lynchings is unrelated to health outcomes. And within the North, residing in a high or low lynching state also made no difference. The main factor driving their result is that health outcomes are worse in the South, even when controlling for a handful of other risk factors.
In the discussion section, the researchers attempt to dismiss these null results by noting that “the high overlap of participants living in U.S. South and a state with high lynching proportions may have induced some collinearity in our fully adjusted models.” Of course, there would be less collinearity if the researchers had not dichotomized the measure of lynchings. Regardless of their explanation, the fact remains that they have null results when controlling for region. This means that health outcomes for black subjects appear to vary based on the region in which they live, not the number of historic lynchings.
The claimed finding that exposure to lynchings of black victims by black subjects causes adverse health outcomes is further undermined by results that are inconsistent with their causal narrative. Specifically, they find that white subjects also have significantly lower cognitive performance in states with above median number of lynchings of black victims in all models except the one that controls for the South that also produces null results for black subjects.
The researchers attempt to explain this unexpected finding by arguing: “it is likely that structural racism against people racialized as Black co-occurred with structural racism-related factors, such as economic underdevelopment, which created a ‘universal harm’ (Brown and Homan, 2024) that also adversely impacted people racialized as White in the U.S. South.” By acknowledging that other factors, such as economic underdevelopment in the South may account for the adverse health outcomes of white subjects, it is unclear why this could also not be the explanation for the negative outcomes for black subjects.
Lastly, the claim that these subjects would have been exposed to lynchings strains credibility given how almost 99 percent of lynchings occurred before the average subject in the study could have been aware of them as a child. The average age for black subjects in the study was 67.68 when baseline data was collected in 2006 or 2008, meaning they were born around 1939. After 1942, when these subjects would have been three years-old, there were only 26 lynchings with black victims recorded nationwide in the Tuskegee Institute data set used by the researchers. That means that over 99 percent of the lynchings with black victims used for the study’s analysis occurred before the average subject could have been aware enough to have “experienced” it.
The only way that black subjects could have been affected is by living in the kind of state that had previously witnessed lynchings of black victims. But just as economic development is a different causal mechanism than the stress of having experienced lynchings, the conditions that facilitated lynchings in certain states before subjects could have been aware of those events are not the same thing as lynchings themselves.
All that this study demonstrates is that black and white subjects in the South have worse health outcomes than subjects in other regions. We have no way of knowing whether lynchings, economic conditions, or other factors in the past or present contributed to these negative health results. Claiming that the stress of experiencing lynchings caused these health problems is without any scientific basis. No credible scientists would use this evidence to make that claim and no credible scientific journal would publish and stand by these results. No credible health agency should be funding this pseudoscience, either.
[i] In another example of sloppiness, the article twice describes the effects as 18.5%: “Black that lived in states with higher proportions of lynchings (in midlife) experienced 18.5% (95% CI 3%, 36%) higher circulating CRP levels than participants racialized as Black that lived in states with lower proportions of lynchings.” But the coefficient in Table 3 is .17 and .185 does not appear anywhere in the tables of results.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_1904068345-scaled.jpg17072560Laura Morganhttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngLaura Morgan2025-03-14 19:10:152026-05-11 13:46:02The Quackery of Columbia’s Racialized Medical Research
RICHMOND, VA; March 12, 2025 – Today, Do No Harm announced support for the Children’s Hospital GME Support Reauthorization Act that Representative Dan Crenshaw will introduce in Congress. This act will block funding for graduate medical education programs at children’s hospitals if the hospital provides sex change procedures for minors.
Since 1999, the Children’s Hospital Graduate Medical Education (CHGME) program has funded graduate medical education programs to train resident physicians and dentists. The Children’s Hospital GME Support Reauthorization Act of 2025 extends the CHGME program through 2030. The legislation prevents CHGME funding from going to hospitals that administer child sex change interventions such as cross-sex hormones, puberty blockers, and surgeries.
“The American taxpayer should not fund hospitals that perform unscientific sex-change procedures on minors,” said Dr. Kurt Miceli, Medical Director at Do No Harm. “Representative Crenshaw’s bill is important to help protect our children by ensuring federally-funded graduate medical education programs do not engage in these harmful practices. Do No Harm supports this bill to help restore true quality of care, faith and trust in our profession. We thank Representative Crenshaw for introducing it.”
“We’re standing for basic medical ethics and recognizing those who have been silenced and betrayed by a system that put ideology ahead of genuine care,” said Representative Dan Crenshaw. “Medicine should be grounded in truth and healing—not in false promises that cause lasting harm. I will always fight for detransitioners and push for real safeguards to ensure no one is harmed by dangerous gender transition procedures in the future.”
Do No Harm, established in April 2022, has rapidly gained recognition and made significant strides in its mission to safeguard healthcare from ideological threats. With 16,000 members, including doctors, nurses, physicians, and concerned citizens across all 50 states and 14 countries, DNH has achieved over 10,000 media hits in top-tier publications and garnered widespread attention through numerous broadcast news appearances.
https://donoharmmedicine.org/wp-content/uploads/2022/11/DNH_ContentCards_PressRelease.png6751200Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-03-12 16:22:422026-02-11 15:34:00Do No Harm Supports Rep. Crenshaw’s Bill to Stop Funding Hospitals Performing Child Sex Changes
Last week, the Trump administration took another step toward disincentivizing the harmful practice of so-called “gender-affirming care.”
In an executive order, President Trump directed Department of Education officials to exclude “individuals employed by organizations whose activities have a substantial illegal purpose” from public service loan forgiveness.
Per the order, “substantial illegal purpose” includes actions such as “the chemical and surgical castration or mutilation of children or the trafficking of children to so-called transgender sanctuary States for purposes of emancipation from their lawful parents.”
This means that individuals who work at organizations performing child sex changes are not eligible for student loan forgiveness.
Enabling student loan forgiveness for these individuals is a roundabout, indirect subsidy for the practice of so-called “gender-affirming care,” and a boon to the organizations performing these procedures.
Taxpayers should not be on the hook for harmful medical interventions that are not supported by scientific evidence.
This action follows on the heels of a January executive order halting taxpayer funding of these procedures through federal grants and health benefit programs, and directing federal agencies to take appropriate action to restrict access to child sex change interventions.
The January order, which is currently being challenged in the courts, also directed the Department of Justice to “prioritize investigations and take appropriate action to end deception of consumers” relating to the long-term effects of transition drugs and procedures.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_2502569527-1-scaled.jpg15362560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-03-12 11:49:322026-05-11 13:45:40Trump Executive Orders Bars Student Loan Forgiveness to Providers of Child Sex Changes
The University of Arizona College of Medicine at Tucson has quietly removed large chunks of its website overtly pledging support for diversity, equity, and inclusion (DEI).
At first glance, this would seem to be good news. But a closer review indicates this is more a rebrand than a significant shift in institutional posture.
According to archives of the College of Medicine’s website, the school listed a “Diversity and Inclusion” office under its administrative offices up until February 14.
However, at some point between February 14 and today, the Diversity and Inclusion office was removed from the listed administrative offices. In its place is the Access, Community and Belongingoffice.
Additionally, at some point in 2024, the link to the Diversity and Inclusion office began to redirect to the Access, Community and Belonging office before the Diversity and Inclusion office was completely and officially removed.
The webpagefor the older Diversity and Inclusion office appears nearly identical to the version of the webpage for the Access, Community and Belonging office that existed before February 14, and the offices are run by the same administrative official, Celina Valenzuela, MD.
In its effort to rebrand its DEI efforts, the College of Medicine scrubbed several DEI resource pages from its website; they are no longer accessible via the Access, Community and Belonging office webpage.
These include the school’s diversity statement, which pledged to advance diversity through “educating, training, and employing diverse faculty, staff, and student body” and “encouraging and supporting culturally responsive scholarly activities that acknowledge and respect systems of healing that emerge from different traditions.”
Additionally, the school scrubbedits DEI “Recruitment” section that advertised its DEI scholarship – open to “underrepresented” students.
The DEI “Retention” page is also removed, as is the “Obtaining DEI Credits” page that recommends DEI trainings on topics including microaggressions and implicit bias. The section further recommends faculty and staff take the Implicit Association Test to better understand their implicit biases. (Of course, the Implicit Association Test is not predictive of real-world behavior or prejudice.)
However, some vestiges of overt DEI and discriminatory practices remain.
Take the Spurring Success for Women in Medicine & Science (SSWIMS) fellowship, which makes it clear who the school has in mind for the award: “Women, groups underrepresented in medicine and science, and candidates who are diverse in other ways are encouraged to apply.”
Ultimately, it appears this rebrand is an attempt to publicly downplay the school’s more explicit endorsements of DEI ideology while still retaining its substance. The University of Arizona should instead ditch its DEI programs altogether.
https://donoharmmedicine.org/wp-content/uploads/2025/03/shutterstock_2267507097-scaled.jpg19172560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-03-11 22:22:132026-05-11 13:41:46University of Arizona Med School Quietly Rebrands Its DEI Office
According to an open letter spearheaded by Psychologists Against Antisemitism, the American Psychological Association (APA) is failing to address “virulent antisemitism within its ranks.”
The lettercites numerous examples of antisemitic statements and messages in internal listservs; these include statements like “Kudos to Hamas” and calls for “Intifada, Intifada,” as well as calls for Boycott, Divestment, and Sanctions against Israel.
The letter then accuses the APA of failing to properly address this rampant and pervasive antisemitism within its organization, noting its “relative silence” on the issue of antisemitism.
It’s simple: there is no place for antisemitism in the psychology profession. Mental health professionals should all agree that the APA must protect its Jewish members and the Jewish community at large from this disgusting rhetoric.
Help hold the APA accountable and add your name to the letter through the form linked here.
Additionally, the letter cites statements made by Dr. Lara Sheehi, president of the APA Society of Psychoanalysis and Psychoanalytic Psychology (Division 39), that the letter argued equated support of Israel’s right to exist with “psychosis.”
The letter calls on the APA to address and investigate this antisemitic rhetoric and ensure that material harmful to Jews is not part of any continuing education offerings.
As of late February, the letter already had over 3,500 signatures.
Sign on to the letter through the form linked here, and help hold the APA accountable.
https://donoharmmedicine.org/wp-content/uploads/shutterstock_558908494-scaled.jpg17072560Ailan Evanshttps://donoharmmedicine.org/wp-content/uploads/DNH_Logo_Stethescope-1.pngAilan Evans2025-03-07 18:34:162026-05-11 13:39:53APA Accused of Failing to Address Rampant Antisemitism ‘Within Its Ranks’